
Date: 28.11.19
Duration: 1500-1600
Venue: Marjon Sports Therapy Clinic
Reflective Summary:
I booked an hour in the Marjon Sports Therapy and Rehab clinic so that any members of the swimming and water polo teams, could come and see me for assessment of MSK issues or for a massage. My objective is to develop a culture within the team of injury prevention not cure.
Subjective Assessment:
My client was a 20-year old female water polo player. Her general health was good but she is currently under treatment of an osteopath for a suspected disc bulge in lumbar spine. She had an X-Ray of her lumbar spine during the summer of 2019 but there were no issues detected at the time.
Red flags/contraindications:
There are no Cauda Equina or VBI symptoms.
There were no THREADS red flags.
24-hour behaviour:
Left ankle feels fine at the moment.
No early morning stiffness
Aggravating/easing factors
Swimming aggravates condition and rest eases it.
Walking and running is fine and she is still able to play netball.
History of Present condition:
Mechanism: sprained ankle playing netball training 4/52
Onset: Pain immediately after incident. Pain went away, there was no bruising but there was inflammation. Received Game Ready Cryotherapy treatment in the Sports and Rehab clinic 3 days later. The condition eased after 2 weeks of rest and a further 2 weeks of enforced rest because of vertebral discomfort in her lumbar spine.
Previous injuries: The client has sprained her ankle in January 2019 and again 3/12 ago.
She has not been prescribed or is currently taking any medication.
Psycho/Social factors: She has lots of exam/degree stress. She is not currently able to do her external placements because of her lower back issue which is a suspected disc bulge – bilateral.
Objective Assessment
I cleared the knee joint (left & right legs) – active mvmts (flexion, extension, internal and external rotation) with overpressure. There were no issues.
During palpation of the left foot I detected a raise in the tissue underneath the lateral malleolus and it was tender to touch.
AROM
Right foot: no pain during dorsi flexion, plantar flexion, inversion and eversion.
Left foot: client felt pain during plantar flexion and a pulling sensation – 4/10, and pain in inversion 5/10. No pain in dorsi flexion or eversion.
PROM
Right foot: full ROM in all mvmts
Left foot: pain in plantarflexion and inversion but ROM was not restricted. A sports therapy lecturer demonstrated how to apply combine the passive mvmts of plantarflexion and inversion rather than doing them as two separate movements.
Resisted ROM
Right foot: full strength in all mvmts
Left foot: weakness in plantarflexion 4/5 and inversion 4/5
The client also demonstrated weakness in plantar flexion during a single-leg heel raise.
Special Tests
+ve Anterior Draw Test for ATFL
+ve Talar Tilt test for CFL – with foot in anatomical position
+ve Talar Tilt test for ATFL – with foot relaxed
The results of the assessment confirmed that there was damage to the lateral ligament complex. Initially I believed that it was the ATFL however the +ve Talar Tilt test and the inflammation and tenderness of the tissue underneath the lateral malleolus confirmed that the issue was actually the CFL.
Treatment:
A programme of prescribed exercises to improve strength and proprioception was devised for the client as follows:
2 3 sets of the exercises below to be repeated twice per week
8 reps of heel raises on the floor – to be performed slowly (2 counts up, 2 counts down)
8 reps of heel raises with a theraband around the ankles – to be performed slowly (2 counts up, 2 counts down)
8 reps of a single-leg Y balance.
I described and demonstrated the exercises to the client and encouraged her to practise them to ensure that she was clear on how to perform them.
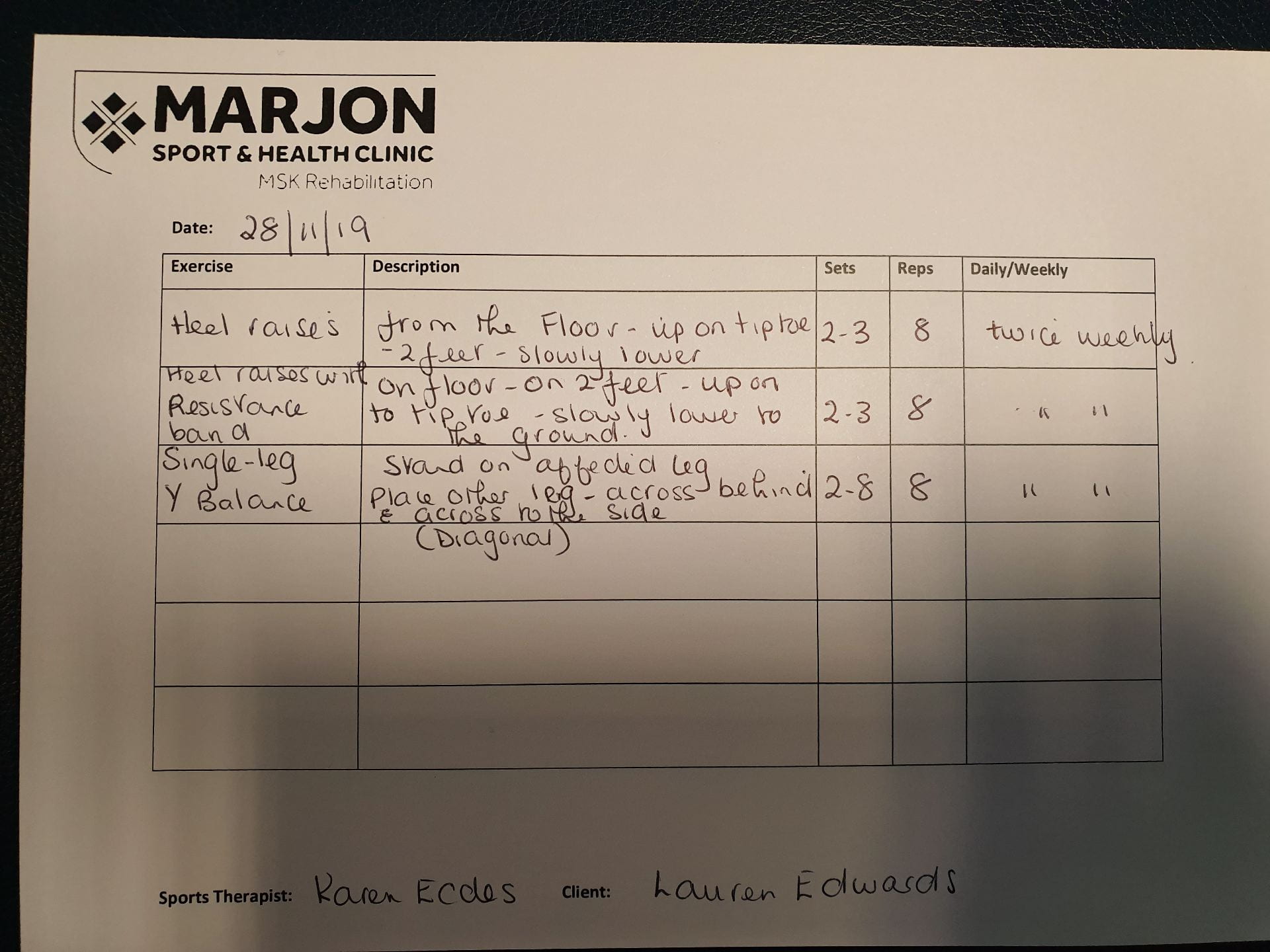
Figure 1 – Programme of exercises to improve strength & Proprioception
A rigid taping was applied to the ankle as follows:
2 x C strips applied above the malleoli
2 x figure of 6 strips applied
2 x stirrups strips applied with a stretch on the lateral side to provide support
2 x C strips to complete and secure the taping.

Figure 2 – Figure of 6 rigid taping
I really enjoyed going through the subjective and objective assessments with the client and gained. It gave me some confidence going through the assessment process on my own. I developed a nice rapport with the client and was positive and supportive throughout. I need more practise apply the rigid tape as it can be quite tricky.
Areas for further improvement plus action plan
Practise passive movements of the ankle and think about joining movements together.
Practise rigid taping.
Returning to reflections at a later date