Running total of hours: 98
Patient 1 – Patient Overview: This patient is a student therapist and presented with acute and severe back pain and neurological symptoms of sciatic down his left side. Sudden Onset 2 hours after volleyball training after sitting down. Very restricted in all ROM and experiencing 9/10 levels of pain.
Neurodynamic are still a weak area of my knowledge and understanding and so the practical application of testing and treatment is a real challenge for me within my practice. I am confident in the methods used to test for lower back neurological dysfunction but I am not able to interpret these findings or follow through an effective, thorough assessment that boasts accuracy or specificity.
My supervisor helped to work through the assessments for root nerve impingements, but even when observing, I was unable to fully appreciate the mechanisms used and outcomes observed. I also find treatment in response to findings very challenging.
The Straight Leg Raise is performed as demonstrated by the Physio tutors:
https://www.youtube.com/watch?v=LdAD9GNv8FI
According to a review by Capra et al. (2011) the straight leg raise was not found to be an effective in identifying lumbar disc herniations with a sensitivity of 0.36 and a specificity of 0.74.
Two other commonly used neurodynamic tests for lower limb pathological neuropathy are as follows and are useful tools in the assessment of patients with symptoms with radicular leg pain indicating nerve root impingement or lumbar disc herniation.
The Slump Test as shown in the following video by the Physiotutors, has been shown to have a sensitivity of 0.91 and a specificity of 0.70 (Urban & Macneil, 2015):
https://www.youtube.com/watch?v=HFGfP84uwEo
And the Prone Knee Bend as demonstrated in this video by the Physiotutors.
https://www.youtube.com/watch?v=4VxKyPRq6HA
These two tests alone have reasonable sensitivity and specificity, however in research conducted in a pilot study by Trainor & Pinnington (2011), a technique known as the slump knee bend test as shown in figure 1 is a variation on the prone knee test and found to have a sensitivity of 1.00 and specificity of 0.83 at identifying lumbar root compression at L4. Although it was noted that this test may not be able to identify compression at other lumbar locations, it is recommended as a slightly more reliable test for the presence of neurological pathology and as such could be used in conjunction with other neurodynamic tests. The test was carried out as shown in Figure 1.

From these tests we found positive signs and indicators of nerve root impingement, but I was unsure as to how to treat my patient based on these findings. Because of the acute nature of the injury, the likelihood of muscle guarding and spasms and the intensity of pain, it would have been difficult to fully assess this patient at this session. I did, however, apply STM to his lower back to help relieve tension from the surrounding soft tissue and to help relieve the pain. The patient was advised to return to the clinic for some traction to decompress the spine in an attempt to reduce pain and improve function in the lumbar spine with research suggesting that traction even in the form of the straight leg raise with added traction is an effective treatment modality, especially when combined with other treatments such as home based strengthening exercise programs (Cho, Lee and Hwangbo, 2015; Gǔlşen, Atici, Aytar and Sahin, 2018; Meszaros et al., 2000; Pawar & Metgud, 2014). It is useful to know that in the absence of a traction machine or if the patient was of large body size, posterior to anterior mobilisations have also been found as equally effective as traction with straight leg raise. Another pain relief option that I did not consider but are recommended could be the use of a TENS machines (Pawar & Metgud, 2014).
Fortunately, however this clinic has a mechanical traction machine which is readily available and as such proved very useful in this particular case with this treatment being found to significantly change pain levels and function in patients with nerve root compression when 12 treatments were performed over 6 weeks.
According to NICE Guidelines, as summarised by Bernstein Malik, Carville and Ward (2017), manual therapy and exercise programs were advised as well as other modalities such as stretching and mobilisations, all of which I will hope to incorporate into a rehabilitation program for the patient as the acute nature of the injury subsides.
Patient 2 – This patient presented with lateral knee pain with the clinical subjective notes as follows;
Started running in January 11/24 ago, couch to 5km. increasing mileage and groups. Started getting “niggles” in ankle, no niggles since 3/12 ago.
Off road event, slipped and now sharp pain in knee. 5 days of Px now fine. Has had week off running.
Was recommended a sports massage. Booked 2/52 ago.
10km, training for 1/2 marathon. Increasing running, 11.5miles.
Currently 25miles/week.
1/52 ago Px in lat. R knee. Px in morning, eases through day, Px again in evening.
Running stabbing Px 7/10, had to stop running. Now no Px.
Stairs Px going down stairs.
Px when injury at worse. OK now.
Although this patient had requested a sports massage, it became apparent early on in the subjective assessment that this modality alone would not prove the most effective in this case and a more comprehensive assessment was required. As the patient was unsure as to the nature of a sports massage and visited the clinic with the clear objective of an injury diagnosis or treatment, I continued to perform a full assessment instead.
From an objective assessment, I noted that the patient had significant pes planus in the same foot as his knee pain. Pes planus is a common foot deformity also known as flat feet and is commonly caused by weakness in the surrounding muscular, such as the plantar and dorsiflexors, inverters, and evertors, but more specifically the tibialis posterior muscles, which, when weakened can present with a condition recognised as posterior tibial tendon dysfunction (Erol et al., 2015).
According to a findings from a study by Lee & Choi (2016) and Ashford, Mathieson and Rom (2016) strengthening exercises of the foot intrinsic muscles and tibialis posterior were effective in treating possible causes or symptoms of pes planus by way of reducing foot stability, plantar pressure and balance with an administered rehabilitation program of six weeks included five 30minute sessions. It has also been reported in a study on runners in particular that strengthening of the intrinsic and extrinsic foot muscles is an effective treatment modality for individuals with pes planus who present with associated overuse injuries (Ridge et al., 2018).
During the session I attempted to demonstrate an exercise to help strengthen the patient’s arches but failed terribly; the movements of arch squeezes are subtle and difficult to explain and as such I did not feel as though the patient was confident in his understanding of the exercises.
I have since been able to find some more exciting exercises to use for patients to do and hopefully with a little more enjoyment too, which may also help to increase exercise adherence.
Exercises such as picking up objects with feet, folding clothing or towels with feet and walking on the lateral side of feet were suggested by Erol et al. (2015) as well as the more-simple resistance band exercises and toe heel walking.
Shadowing Ankle Taping
In between patients, I decided to shadow another therapist who was treating a patient as part of his placement with the Marjon University Netball team. This patient had suffered a mild ankle sprain two weeks prior to this session and was hoping to return to training today, but with appropriate level of participation. In order to take part, additional support by means of rigid ankle taping was applied, the method used was that of the figure of 8 shown in the video below and as used in a study by Halim-Keranegara, Raymond, Hiller, Kilbreath and Refshauge (2017) and in figure 1.
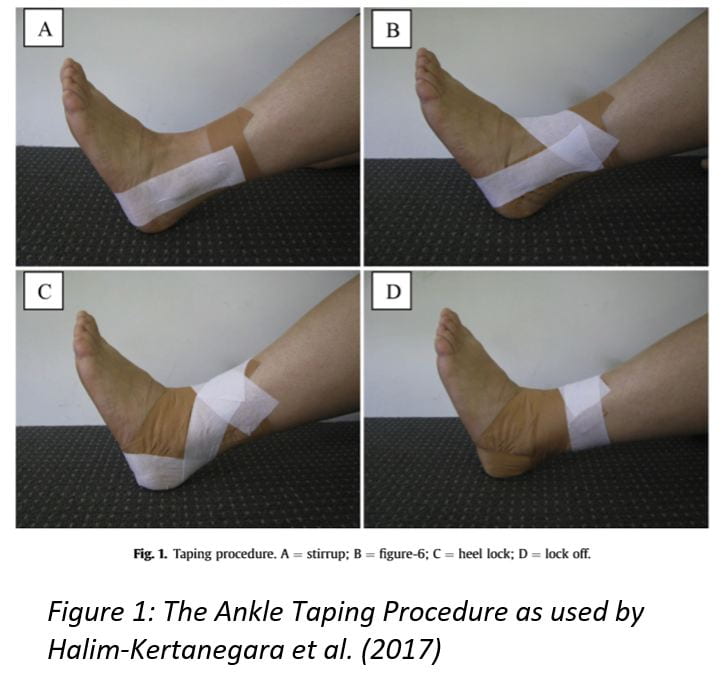
https://www.youtube.com/watch?v=16lF6hOB4bs
Although the effects of ankle taping by way of mechanical support has been widely disputed, with studies suggesting it as beneficial such as Kuni, Mussler, Kalkum, Schmitt and Wolf (2016) and those that have found it is not, such as Jaffar et al. (2016), there are some other benefits beyond these physical effects. Psychological elements, including an athlete’s perceived ability to perform and self-efficacy were reportedly improved after mechanical taping was applied and as such the use of tape may be useful in aiding a quicker return to sport (Halim-Kertanegara et al., 2017).
The therapist used non elastic rigid taping for this procedure but as reported by Abián-Vicén, Alegre, Fernández-Rodŕiguez and Aguado (2009), with the same supporting effects, elastic taping has been found to be more comfortable and less restricting but without compromising the mechanical effects of the tape. The patient was quick to complain about the discomfort, not in her ankle, but by the feeling of the tape, so this study was able to provide evidence for the use of a more comfortable alternative. In future, if mechanical support is my objective then this taping may be slightly more comfortable.
It is thought that kinesiology tape is an effective treatment to help improve functional performance in the ankle, help improve balance and proprioception and help prevent lateral ankle sprains (Jackson, Simon and Docherty, 2016; Lee & Lee, 2016; Y. Wang et al., 2018). One of the physiological effects of the tape is the neurological responses from the mechanoreceptors in the ankle with tape; the feeling of the tape on the ankle becoming a more efficient stimulus for quicker muscle reaction times of the peroneals in particular and in individuals with chronic ankle instability, either caused by or which has caused muscle weaknesses in the ankle. Research by Jaffar and Li (2016) for example, found greater increases in muscle activation of the peroneal longus muscle during dynamic movements in subjects with functional ankle instability with the presence of rigid tape compared with subjects with kinesiology tape or no tape.
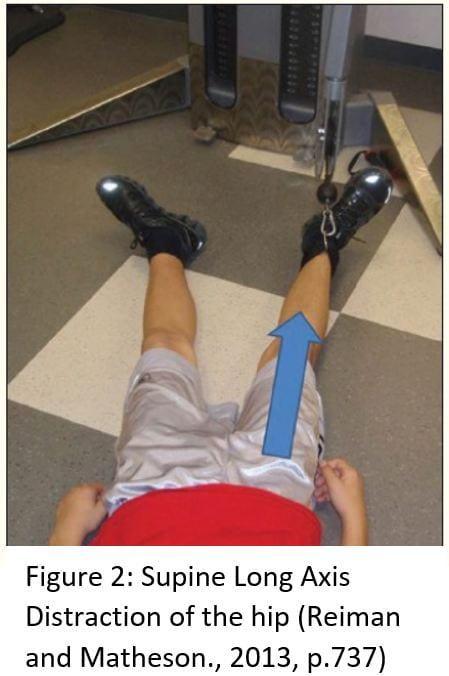
Patient 3 – This patient presented with Lower back and with a prevalence of up to 33% in the general population (Kachanathu, Alenazi, Seif, Hafez and Alroumim, 2014), this patient is one of many who I come across for soft tissue therapy treatment in the clinic. I treated this patient with evidence based deep tissue massage and mobilisations as well as prescribing a suitable exercise and stretching program to help strengthen and maintain more pain free ROM (Kachanathu et al., 2014; Shah & Kage, 2016). However, what I found most interesting in this case was the request for traction of the hip by way of unilateral pulling of each leg at the ankle. It has been found that treatment aimed at the hip joints are effective in the management of chronic lower back pain (Burns, Mintken, Austin and Cleland, 2011). This patient self-reported improvements in his symptoms after this treatment. I have performed traction type mobilisations to the SI Joint at my external placement and have developed an effective technique for this, but this was my first experience of traction of the hip.
In order to perform this, I grasped the patient’s ankle and pulled, producing and longitudinal distraction of the hip and repeated this on both legs. This method has been suggested for patients who require a general stretch of the hip joint capsule (Reiman & Matheson, 2013). Figure 2 is a version of this distraction technique that can be performed at home so the patient can continue with this treatment at home to maintain progress and reduced levels of pain in between the treatment sessions.
Patient 4 – This patient was a follow up from the previous week (Patient 3, Tuesday 5th November). Nothing has changed from the previous week of treatment for possible achillies tendinopathy but as we ran out of time for STM, she had returned to receive this. As I forgot to test any objective measures, before I performed treatment as used in Stefansson, Brandsson, Langberg and Arnason (2019), I made sure to carry out the knee to wall test, which showed bilateral shortening in both legs and a significant inability to gain a reasonable distance from her foot to the wall, indicating the need to increase either joint mobility or probably more likely, the presence of gastrocnemius and soleus dysfunction by way of reduced length or flexibility. There is an abundance of research on the methods of achillies tendon rehabilitation, however they are often conflicting and are continuing to develop. Sports massage treatments and programs including eccentric and/or concentric exercises have been studied and reviewed, with eccentric exercises most often the more preferred option. Research conducted by Malliaras et al. (2013), for example found that no one method is more effective than the other but suggested eccentric-concentric as a foundation of treatment. This study, along with many other, highlight the need for further research into the mechanical effects of various loading programs; a possible reason why treatment methods remain undecided. A more recent study by Chaudhry, Morrissey, Woledge, Bader and Screen (2015) found that eccentric exercises were more effective than concentric exercises of the triceps surae muscle group in the rehabilitation of achillies tendinopathy but other studies within that same year found either method to be equally as effective with no significant differences between subject groups (Beyer et al., 2015). A single-blind randomised control study on the effects of massage on achillies tendinopathy by Stefansson et al. (2019) reported that a commonly accepted risk factor for achillies overuse injuries is muscular tightness in the triceps surae group and associated reduction in ankle ROM. Furthermore, although eccentric strengthening is widely reported as the most effective treatment for this injury, this study found that pressure massage was as effective as eccentric exercises and potentially allowed for a quicker resolution in symptoms, as this modality can result in earlier and more immediate effects. Interestingly, however, this research did not find reason to combine the two treatments as further effects of this were not significantly increased.
In order to maintain the effects of the STM at home, I suggested that the patient use a foam roller at home on a daily basis, as this has been found to be effective in reducing muscle pain and increasing flexibility (Wiewelhove et al., 2019).
This session was also a good opportunity to ensure that the patient was performing the prescribed exercises with the correct routine, having had a week to get to grips with the program and discover any areas that may not have been fully understood. Often, patients rebook appointments for weeks ahead and as such, any issues with the prescribed programs cannot be addressed early enough. In this case, the patient queried the side lying abductor exercise (prescribed for suspected weakness in the hip abductors) as she was unsure as to whether her hips should be pushed forward or allowed to drop back; I informed her that in order to isolate the Gluteus Medius muscle, the hips must be pushed forward, as opposed to relaxing the hip back, which activates the Tensor Fascia Latae muscle. In order to ensure that the correct muscles are being used, I instruct the patient to place the tips of their fingers over their Gluteus Medius muscle so that they can feel it contracting during the movement.
Spare time between patients – as neurodynamic testing is a significant area of weakness for me, both in knowledge and practice, as well as the researching behind these, I was able to practice with a partner as fortunately the clinic with busy but with some cancelled appointments. Talking through procedures and methods with other students always seems to take longer than when we are shown directly from the clinic manager or from a lecturer, however by trying to figure out how to do something ourselves, we learn all of the way not to do it and have to understand the practice better in order to understand how it works. I find this time between patients incredibly useful and if there are other students around to help, they are always able to add their own strengths to our practice and they are always willing to help.
References –
Abián-Vicén, J., Alegre, L. M., Fernández-Rodŕiguez, J. M., & Aguado, X. (2009). Prophylactic ankle taping: Elastic versus inelastic taping. Foot and Ankle International. https://doi.org/10.3113/FAI.2009.0218
Ashford, R., Mathieson, I., & Rome, K. (2016). Conservative Interventions for mobile Pes Planus in Adults: a systematic review. Revista Internacional de Ciencias Podológicas. https://doi.org/10.5209/rev_ricp.2016.v10.n2.52304
Bernstein, I. A., Malik, Q., Carville, S., & Ward, S. (2017). Low back pain and sciatica: Summary of NICE guidance. BMJ (Online). https://doi.org/10.1136/bmj.i6748
Beyer, R., Kongsgaard, M., Hougs Kjær, B., Øhlenschlæger, T., Kjær, M., & Magnusson, S. P. (2015). Heavy slow resistance versus eccentric training as treatment for achilles tendinopathy: A randomized controlled trial. American Journal of Sports Medicine, 43(7), 1704–1711. https://doi.org/10.1177/0363546515584760
Burns, S. A., Mintken, P. E., Austin, G. P., & Cleland, J. (2011). Short-term response of hip mobilizations and exercise in individuals with chronic low back pain: A case series. Journal of Manual and Manipulative Therapy. https://doi.org/10.1179/2042618610Y.0000000007
Capra, F., Vanti, C., Donati, R., Tombetti, S., O’Reilly, C., & Pillastrini, P. (2011). Validity of the straight-leg raise test for patients with sciatic pain with or without lumbar pain using magnetic resonance imaging results as a reference standard. Journal of Manipulative and Physiological Therapeutics. https://doi.org/10.1016/j.jmpt.2011.04.010
Chaudhry, S., Morrissey, D., Woledge, R. C., Bader, D. L., & Screen, H. R. C. (2015). Eccentric and concentric exercise of the triceps surae: An in vivo study of dynamic muscle and tendon biomechanical parameters. Journal of Applied Biomechanics. https://doi.org/10.1123/JAB.2013-0284
Choi, J., Lee, S., & Hwangbo, G. (2015). Influences of spinal decompression therapy and general traction therapy on the pain, disability, and straight leg raising of patients with intervertebral disc herniation. Journal of Physical Therapy Science. https://doi.org/10.1589/jpts.27.481
Erol, K., Karahan, A. Y., Kerimoğlu, Ü., Ordahan, B., Tekin, L., Şahin, M., & Kaydok, E. (2015). An important cause of pes planus: the posterior tibial tendon dysfunction. Clinics and Practice. https://doi.org/10.4081/cp.2015.699
Gǔlşen, M., Atici, E., Aytar, A., & Sahin, F. N. (2018). Effects of traction therapy in addition to conventional physiotherapy modalities on pain and functionality in patients with lumbar disc herniation: Randomized controlled study. Acta Medica Mediterranea. https://doi.org/10.19193/0393-6384_2018_6_315
Halim-Kertanegara, S., Raymond, J., Hiller, C. E., Kilbreath, S. L., & Refshauge, K. M. (2017). The effect of ankle taping on functional performance in participants with functional ankle instability. Physical Therapy in Sport, 23, 162–167. https://doi.org/10.1016/j.ptsp.2016.03.005
Jackson, K., Simon, J. E., & Docherty, C. L. (2016). Extended use of kinesiology tape and balance in participants with chronic ankle instability. Journal of Athletic Training, 51(1), 16–21. https://doi.org/10.4085/1062-6050-51.2.03
Jaffar, M. R., Jaafar, Z., & Li, G. S. (2016). Peroneus longus activity in different types of taping: athletes with ankle instability. Revista Brasileira de Medicina Do Esporte. https://doi.org/10.1590/1517-869220162203142486
Kachanathu, S. J., Alenazi, A. M., Seif, H. E., Hafez, A. R., & Alroumim, A. M. (2014). Comparison between Kinesio taping and a traditional physical therapy program in treatment of nonspecific low back pain. Journal of Physical Therapy Science, 26(8), 1185–1188. https://doi.org/10.1589/jpts.26.1185
Kuni, B., Mussler, J., Kalkum, E., Schmitt, H., & Wolf, S. I. (2016). Effect of kinesiotaping, non-elastic taping and bracing on segmental foot kinematics during drop landing in healthy subjects and subjects with chronic ankle instability. Physiotherapy (United Kingdom). https://doi.org/10.1016/j.physio.2015.07.004
Lee, D., & Choi, J. (2016). The Effects of Foot Intrinsic Muscle and Tibialis Posterior Strengthening Exercise on Plantar Pressure and Dynamic Balance in Adults Flexible Pes Planus. Physical Therapy Korea. https://doi.org/10.12674/ptk.2016.23.4.027
Lee, S. M., & Lee, J. H. (2016). Effects of ankle eversion taping using kinesiology tape in a patient with ankle inversion sprain. Journal of Physical Therapy Science. https://doi.org/10.1589/jpts.28.708
Malliaras, P., Barton, C. J., Reeves, N. D., & Langberg, H. (2013). Achilles and patellar tendinopathy loading programmes: A systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Medicine. https://doi.org/10.1007/s40279-013-0019-z
Meszaros, T. F., Olson, R., Kulig, K., Creighton, D., & Czarnecki, E. (2000). Effect of 10%, 30%, and 60% body weight traction on the straight leg raise test of symptomatic patients with low back pain. Journal of Orthopaedic and Sports Physical Therapy. https://doi.org/10.2519/jospt.2000.30.10.595
Pawar, A. H., & Metgud, S. (2014). “ Comparative Effectiveness of Mulligan ’ s Traction Straight Leg Raise and Bent Leg Raise in Low Back Ache with Radiculopathy ” – A Randomized Clinical. International Journal of Science and Research.
Reiman, M. P., & Matheson, J. W. (2013). Restricted hip mobility: clinical suggestions for self-mobilization and muscle re-education. International Journal of Sports Physical Therapy.
Ridge, S., Henderson, A., Bruening, D., Jurgensmeier, K., Olsen, M., Griffin, D., … Davis, I. (2018). Midfoot Angle Changes During Running After an 8-week Foot Strengthening Program. Foot & Ankle Orthopaedics, 3(3), 2473011418S0040. https://doi.org/10.1177/2473011418s00405
Shah, S. G., & Kage, V. (2016). Effect of seven sessions of posterior-to-anterior spinal mobilisation versus prone press-ups in non-specific low back pain-randomized clinical trial. Journal of Clinical and Diagnostic Research, 10(3), 10–13. https://doi.org/10.7860/JCDR/2016/15898.7485
Stefansson, S. H., Brandsson, S., Langberg, H., & Arnason, A. (2019). Using Pressure Massage for Achilles Tendinopathy: A Single-Blind, Randomized Controlled Trial Comparing a Novel Treatment Versus an Eccentric Exercise Protocol. Orthopaedic Journal of Sports Medicine, 7(3), 1–10. https://doi.org/10.1177/2325967119834284
Urban, L. M., & Macneil, B. J. (2015). Diagnostic accuracy of the slump test for identifying neuropathic pain in the lower limb. Journal of Orthopaedic and Sports Physical Therapy. https://doi.org/10.2519/jospt.2015.5414
Wang, Y., Gu, Y., Chen, J., Luo, W., He, W., Han, Z., & Tian, J. (2018). Kinesio taping is superior to other taping methods in ankle functional performance improvement: a systematic review and meta-analysis. Clinical Rehabilitation. https://doi.org/10.1177/0269215518780443
Wiewelhove, T., Döweling, A., Schneider, C., Hottenrott, L., Meyer, T., Kellmann, M., … Ferrauti, A. (2019). A meta-analysis of the effects of foam rolling on performance and recovery. Frontiers in Physiology. https://doi.org/10.3389/fphys.2019.00376