Running total of hours: 137.5
Unfortunately, this session was somewhat setback by an ongoing lower back issue of mine and so I was not able to fully apply myself physically to administer any manual treatments, however as I really enjoy attending the clinic and feel a responsibility for my patients I did not want to miss the opportunity to treat and attended to gain further practical experience, but with occasional manual help when needed; to start with I worked with another student for 2 patients for the first part of this session until I felt I could manage, offering advice where I could and taking an equal part in the appointments.
Patient 1 – Neck Injury and STM
This patient was a student who rugby player sustained a neck injury during a game one week ago and this was her follow up appointment.
It is reported that concussion, most likely occurring during a tackle, is the most common injury in rugby union (Cross et al., 2019).
Initially I was anxious about assessing a neck injury but by going through her previous notes, I was reassured by her previous appointment with Alex Walker, the clinic supervisor; the notes were thorough and clearly stated the need to revisit A & E, where the patient was further assessed and any serious injury was ruled out.
The first assessment was performed one day after the injury and it was obvious that the patient was concussed. Because of this and coupled with the very acute nature of her symptoms, no tests were performed, however her visit to A & E ruled out any neurological involvement and a thorough test was carried out.
If this was my patient alone, I would probably have subjected her to a full assessment, including any neurodynamic testing of the cervical spine, however the therapist in this appointment chose not to do this based on the absence of any indicative symptoms. I would agree that this is good rationale for not putting this patient through another session of testing, as she had already been subjected to a number of assessments within the week prior to this session and has simply requested a STM.
The muscle testing for this patient was strongly indicative of muscular tension and resultant pain, so this coupled with the mechanism of injury and with the improving nature of the pain and ROM, a deep tissue massage with passive and active passive stretching was performed to help facilitate the increase in ROM.
I often forget to include objective measures within my treatment, but in this instance, because I perform ROM tests as part of the basic assessment, I am able to use this as a marker, as long as I remember to retest at the end of the treatment.
This patient reported increases in pain and ROM after the massage and stretching treatment and as such, we knew that this treatment was the most effective treatment for her and prescribed some further stretches to complete at home, as well as a strengthening program for her to start when ROM is back to full range and when pain has mostly subsided.
We felt confident that this individual would adhere to any home exercise programs prescribed because of her passion to return to rugby and her need to be fit to play again.
We also discussed the importance of taking the advised time off of her sport, due to her concussion. It is important to educate individuals about the dangers and risk factors involved with concussion and to be aware of a number of factors associated with this type of traumatic injury. A study by Bussey et al. (2019) found that neuromuscular control can be altered during rugby tackling within twelve months of sustaining a concussion which can pose as a potential future risk factor for subsequent concussions.
Initially, I had naively thought that by increasing muscular strength of the neck muscles, future injury or concussion risk may be reduced, however a review by Benson et al. (2013) found no evidence in support of this, nor any evidence advocating the use of mouth guards or helmets. A recent study suggested that tackling position and acceleration and speed of the tackler can be altered as a way to reduce the risk (Cross et al., 2019) but these as external factors that are beyond the control of the therapist. From this, the only advice that I was able to offer this patient was to follow guidelines provided by the national governing body of her sport, in this case rugby and to take the suggested time off by the physicians at the hospital.
Patient 2 – STM and Traction at hip
This patient was returning for another session of STM of the back with additional piriformis release and manual hip traction.
After his session three weeks previous, he remarked on his improvements, having felt a significant relief from his usual tension.
After my previous session with this patient on 11th November, I looked into the value of this treatment and ways in which this could be done at home to save his time and money. Reiman and Matheson (2013) supported the use of a home-made device that simply connects the foot with an anchor, such as heavy furniture or gym equipment so that the individuals can apply a long axis distraction force of the hip. I suggested this option to my patient so that he could start to rely less on treatments and self-manage his discomfort, however he immediately responded with his dissatisfaction at any self-performed treatment and explained that he was aware that he could potentially administer his own treatment.
It is in my opinion that as long as the patient is aware of the transient nature of the STM and traction and as long as we, as therapists, provide the patient with exercises to progress through and educate them on their injury and rehabilitation plan, if they continue to want these passive treatments then this is completely justified. It would be unethical, however if I were to provide this basic level of treatment on its own, unaccompanied by a more long term correction and patient education.
I am aware of the short term, transient nature of soft tissue treatment and the need to incorporate strengthening exercises as the most part of any rehabilitation plan for developing and enhancing functional movements, however I am also of the opinion that these two are transient; when exercises are stopped, muscles become weakened again. So, in my view both strengthening and passive soft tissue therapy are transient, the difference is that the patient is more able to perform the strengthening exercises at home and become fully empowered to sustain their own musculoskeletal function, compared with the more specific requirements of STM and the need to see a specialist for a more satisfying experience, as experienced by this patient.
People pay to get their hair or nails treated, but there are no long term benefits of this to their health, so as long as people are attending their appointments knowing that they are receiving treatment to help with their pain and ROM in the short term then I feel like the treatment is entirely justified. We should always provide the patients with information about how they might be able to maintain their function outside of the clinic but also we must be aware that this may be of no interest to some patients and that short term relief is their only need.
Patient 3 – Osgood’s Schlatter’s Disease
This was my first experience of treating a child under 16 and although initially I felt uncomfortable, I soon became more confident and was able to communicate well with both the patient and his mother.
I was aware that I needed to keep my language simple and any complicated jargon to a minimum. I did find myself talking to the patient’s mother on more occasions that I think was necessary however and as such the patient may have felt uninvolved in the assessment procedure. I was able to pick up on this early enough and changed my approach, which soon brought the attention back to the young patient, who may then have felt more empowered in this initial stage in his rehabilitation.
It became apparent early on, just from the subjective assessment that Osgood’s Schlatter’s disease (OSD) was the most likely diagnosis; bony prominence in both tibial tuberosities, pain in all dynamic sporting movements, high volume of exercise, specifically football, pain when kneeling and the age of the patient being 13 (with the most likely age in the develop of this condition being between 10 and 15 (Vaishya, Azizi, Agarwal and Vijay, 2016)). I continued to conduct a throughout assessment, remembering to clear joints above and below and then felt the need to seek additional advice from a supervisor, as this patient was so young.
When the supervisor initially joined us in the assessment process to offer further advice, the first thing mentioned was the bony ‘lumps’ under both of the patient’s knees. It was quite abruptly mentioned that the lumps will stay but the pain will go, to which both the mother and the patient were taken aback. At first I was surprised at their reactions but now understand why this may have caused some distress; the lumps in the patients’ knees are quite obvious and if they had always visualised this to reduce over time, to find out that the lumps would remain, would have come as a shock. I did take the time later in the appointment to explain that some of the prominence may have been down to acute inflammation, effusion and heat and also more obvious due to the lack of muscle tone in the patient’s leg and from this conversation, both the patient and his mother felt more relaxed about this aesthetic element to the injury. In cases where those prominences are extreme, there is a procedure known as closing-wedge osteotomy, which was found to be an effective means of managing the bony prominence on the tibial tuberosity which is formed as a result of Osgood-Schlatter’s disease (Pagenstert, Wurm, Gehmert and Egloff, 2017).
Figure 1 shows the location and aesthetic appearance of the bony prominence of Osgood’s Schlatter Disease, as well as an x-ray image (Vaishya et al., 2016 p.4;p.5).

Interestingly, only 25% of individuals report pain in the tibial tuberosity (Vaishya et al., 2016) so this is not necessarily the only symptom to consider in this condition.
Osgood’s Schlatter’s Disease is characterised by the inflammation of the patella tendon, precisely over it’s insertion into the tibial tuberosity (Vaishya et al., 2016).
Pathogenic risk factors for OSD are vast, with Watanabe et al. (2018) reporting the following all possible contributors to the disease;
1. Height
2. Weight
3. BMI
4. Quadriceps tightness in kicking leg
5. Soleus, gastrocnemius and quadriceps tightness in non kicking, support leg
6. Centre of gravity
7. Medial Longitudinal Arch measurement
It has been found in a study on 20 subjects with a mean age of 13.4 years old, the same age as the patient that stretching of the quadriceps muscles, in particular, the rectus femoris would help to reduce OSD symptoms (Tzalach et al., 2016), however when I performed the Thomas Test it showed nothing but excellent flexibility in the patient’s hip flexors and knee extensors, specifically the quadriceps.
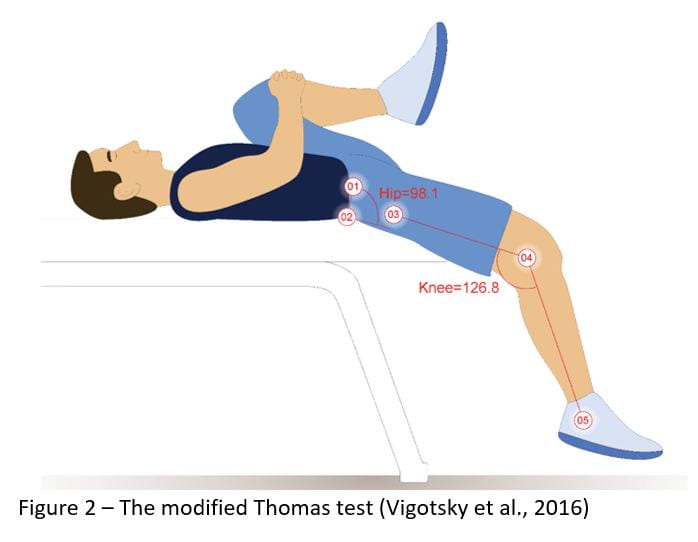
I have since read, however that although the modified Thomas test, shown in figure 1 has been found to be a reliable measure of hip flexor flexibility, it is reliant of a controlled pelvic tilt (Vigotsky et al., 2016).
I do not recall having taken pelvic tilt into account on this occasion, so may not be able to use this as a valid test in this instance unless I retested to account for this variable. However, just from observing, I would be comfortable in suggesting that quadricep flexibility was probably not an issue for this individual.
Instead, we prescribed exercises to strengthen gluteal muscles and hamstrings and educated him and his mother on workload and advised to incorporate plenty of non-sporting days to facilitate his growth but without applying excessive loads. Vaishya et al. (2016) also recommended quadriceps strengthening in addition to the above, so if this patient were to return, I would look to incorporate this element into the rehabilitation program, considering also the lengthened muscles in this case; this may be an indicator of weakness, as opposed to flexibility and I should have taken this into account when assessing this.
With the aim to reduce pain and manage swelling, we advised him to treat any inflammation as and when needed and to continue in his use of ICE and another other relieving modalities, which may also help to reduce the inflammation of the OSD but also of other conditions that may also be present or likely in this particular case, such as patella tendinitis or infrapatellar bursitis, as reported by (Vaishya et al., 2016).
Often, the presence of both of these aforementioned conditions are likely alongside OSD but sometimes these conditions may be the cause of the symptoms but mistaken for OSD; of these, however, it is hard to make an accurate differential diagnosis due to their similar epidemiology and presentation although treatment is often similar (Vaishya et al., 2016). In this case, however, the obvious prominence, an example shown in figure 1, allows for us to assume OSD as the primary condition but be aware of and treat any secondary issues that may arise.
It was also advised that surgery may be viable option, should conservative treatment not be effective and if the condition remains restrictive and debilitating (Vaishya et al., 2016), however this is rare and usually the symptoms reduce or diminish over time and as previously mentioned, only the prominence will remain.
It will be interesting to know whether the symptoms do start to resolve over the coming weeks, in spite of his plan to continue in his activity levels; he seemed (and understandably so) reluctant to reduce his football hours and so progress may be slower. However, with the exercises prescribed and after receiving information on the condition, the patient and his mother may have a better awareness of how they are able to manage the condition, should the symptoms worsen.
Extra Research in my final hour in clinic –
Initially, after his mother informed us that the patient had been taking Non-steroidal Antiinflammatory Drugs (NSAIDS), specifically Advil, in order to continue to play, I was concerned and was unsure as to whether this was the most appropriate course of treatment to take. As I had no prior knowledge on this, I did not provide any further advice to either advocate the use of these or otherwise. However, according to recent research on OSD, NSAIDS are suggested (Kolodychuk, 2018) and as such perhaps a personal choice by parents of which is beyond my scope of knowledge or area to advice.
References –
Benson, B. W., McIntosh, A. S., Maddocks, D., Herring, S. A., Raftery, M., & Dvořák, J. (2013). What are the most effective risk-reduction strategies in sport concussion? British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2013-092216
Bussey, M. D., McLean, M., Pinfold, J., Anderson, N., Kiely, R., Romanchuk, J., & Salmon, D. (2019). History of concussion is associated with higher head acceleration and reduced cervical muscle activity during simulated rugby tackle: An exploratory study. Physical Therapy in Sport. https://doi.org/10.1016/j.ptsp.2019.03.012
Cross, M. J., Tucker, R., Raftery, M., Hester, B., Williams, S., Stokes, K. A., … Kemp, S. (2019). Tackling concussion in professional rugby union: A case-control study of tackle-based risk factors and recommendations for primary prevention. British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2017-097912
Kolodychuk, N. (2018). Tendinosis as the under lying pathology of osgood-schlatter disease: imaging similarities and treatment implications. International Journal of Orthopaedics Sciences. https://doi.org/10.22271/ortho.2018.v4.i1j.97
Pagenstert, G., Wurm, M., Gehmert, S., & Egloff, C. (2017). Reduction Osteotomy of the Prominent Tibial Tubercle After Osgood-Schlatter Disease. Arthroscopy – Journal of Arthroscopic and Related Surgery. https://doi.org/10.1016/j.arthro.2017.02.012
Reiman, M. P., & Matheson, J. W. (2013). Restricted hip mobility: clinical suggestions for self-mobilization and muscle re-education. International Journal of Sports Physical Therapy.
Tzalach, A., Lifshitz, L., Yaniv, M., Kurz, I., & Kalichman, L. (2016). The Correlation between Knee Flexion Lower Range of Motion and Osgood-Schlatter’s Syndrome among Adolescent Soccer Players. British Journal of Medicine and Medical Research. https://doi.org/10.9734/bjmmr/2016/20753
Vaishya, R., Azizi, A. T., Agarwal, A. K., & Vijay, V. (2016). Apophysitis of the Tibial Tuberosity (Osgood-Schlatter Disease): A Review. Cureus, 8(9). https://doi.org/10.7759/cureus.780
Vigotsky, A. D., Lehman, G. J., Beardsley, C., Contreras, B., Chung, B., & Feser, E. H. (2016). The modified Thomas test is not a valid measure of hip extension unless pelvic tilt is controlled. PeerJ. https://doi.org/10.7717/peerj.2325
Watanabe, H., Fujii, M., Yoshimoto, M., Abe, H., Toda, N., Higashiyama, R., & Takahira, N. (2018). Pathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer Players: A Prospective Cohort Study. Orthopaedic Journal of Sports Medicine, 6(8), 1–8. https://doi.org/10.1177/2325967118792192