
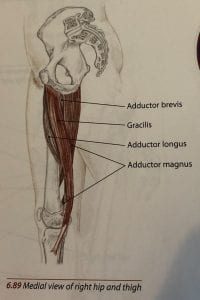
An adductor muscle strain is a tear or rupture to any of the five adductor muscles, which are located in the medial compartment of the thigh (Sathe, 2017). This includes the pectineus, adductor magnus, adductor longus, adductor brevis and gracilis (Eckard et al., 2017). Groin injuries make up 2-5% of all sport-induced injuries, where an adductor strain is usually the musculoskeletal aetiology of the pain (Sathe, 2017). In-between the tendon and bone of the muscle, there is an area that is characterised by a poor blood supply, which triggers a high level of perceived pain and poor healing in adductor strains (Sathe, 2017). These injuries are most commonly reported in sports when the muscles are activated during kicking, twisting, sudden directional changes and rapid accelerations and decelerations (Engebretsen, Myklebust, Holme, Engebretsen, & Bahr, 2010).Athletes are at risk of an adductor strain, especially if they play football, rugby, ice hockey or cricket (Whittaker, Small, Maffey, & Emery, 2015). Furthermore, the prevalence of these injuries has risen from 16thto 4thplace as the most common training injury in Rugby Union (Ryan, Mc Creesh, & De Burca, 2014). When considering sex differences in adductor injuries, the rate of injury to this region was higher in men than women, although this is limited to football (Eckard et al., 2017). In order to develop effective prevention strategies for adductor strains, risk factors need to be identified (Esteve, Rathleff, Urrútia, & Thorborg, 2015).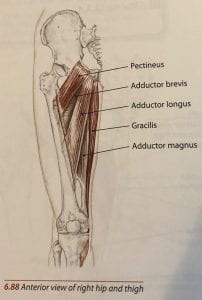
Sports injury risk factors are described as something that contributes to the occurrence of injury in athletes (Ryan et al., 2014). They can be considered intrinsic (person related) and extrinsic (environment related), as well as modifiable or unmodifiable (Spörri, Kröll, Amesberger, Blake, & Müller, 2012). Modifiable risk factors (strength imbalance, muscular tightness) can be changed in order to decrease injury rates by using prehabilitation programmes, where as non-modifiable factors (previous injury, age) cannot be altered (Liu, Garrett, Moorman, & Yu, 2012). Even though non-modifiable factors are unchangeable, they are particularly important in identifying populations that are at an increased risk of injury, therefore prevention strategies such as an exercise prescription can be directed towards people that need it most, such as the elderly (Cameron, 2010). An exercise prescription is a recommended programme of specific fitness related activities that are designed to meet an individual’s health and physical fitness goals, while considering the client’s health status and function (American College of Sports Medicine, 2013). It usually adopts the FITT-VRP principle that includes considering frequency (how long), intensity (how hard), time (duration), type (mode or what kind), volume (amount) and progression (advancement) (Zaleski et al., 2016).
Previous groin injuries are identified as the most common intrinsic risk factor in the literature (Engebretsen et al., 2010). Injury data over a series of consecutive seasons found that footballers are at a 2.4 times greater risk of sustaining an adductor strain, than players who have had no previous history of this injury (Whittaker et al., 2015). This risk factor is significant as reinjuries have found to have longer recovery periods than index injuries, hence reinjury is difficult but critical to prevent (Eckard et al., 2017). Therefore, there needs to be increased attention towards preventing previous injuries from reoccurring, as the vicious cycle of injury and re-injury will not only result in reduced performance and missed training, it can ultimately lead to chronicity and the end of an athletes’ career (Esteve et al., 2015)(Whittaker et al., 2015).
Weak adductor muscles are significant risk factors in terms of absolute strength and when comparing them to the abductors (Engebretsen et al., 2010). Decreased levels of hip adductor strength can result in imbalances between the hip abductor and adductor muscles, reduced muscle capacity and an increased risk of injury during rapid acceleration/deceleration, quick directional movements and striding (Whittaker et al., 2015). These strength imbalances can be between the propulsive muscles, the stabilising muscles of the hip and pelvis and between the synergistic muscles for both the abductors and adductors (Engebretsen et al., 2010). This was supported by O’Conner (2004), whose results implied that uninjured players had higher peak torques in hip adduction compared to those that sustained an injury.
Another risk factor for an adductor strain is core stability (Sathe, 2017). It has been suggested in the literature that reduced core stability was identified if the athlete had delayed contraction of the transverse abdominus (Engebretsen et al., 2010). Similarly, Cowen et al. (2004) found that the transverse abdominus function is altered in patients with adductor related groin pain and that pelvic instability may be another risk factor for this injury (Weir et al., 2010). Therefore, an exercise prescription including core stability needs to implemented in order to reduce and prevent the risk of re-injury to the adductor muscles.
Literature supports the association of lower levels of sport specific training and pre-season sports specific training, as a risk factor for adductor strains (Ryan et al., 2014). Pre-season training is essential, as it could allow both muscular weaknesses and imbalances to be addressed, in order for muscles to be utilised more effectively, enabling less muscular fatigue (Whittaker et al., 2015). Ultimately, if there is reduced sport specific training, the athlete is more susceptible to injury, especially when faced with increased training loads, once the season has begun (Buchheit et al., 2013).
Other potential risk factors include a high level of play, age, reduced range of movement (ROM) in hip abduction and femur diameter (Engebretsen et al., 2010). The reason there is risk linked to ability is because a professional will more than likely work at a higher intensity in training and matches, as well as participate in a greater number of training hours, therefore is more likely to get injured (Whittaker et al., 2015). As players get older, collagen becomes less elastic, meaning it is less able to respond to and absorb forces or recover from fatigue (Ryan et al., 2014). Similarly, Johnson, Mille, Martinez, Crombie and Rodgers (2004) found physiological evidence that abduction to adduction torque decreases with age. Hip abduction ROM and total hip rotation range have been identified as risk factors for adductor injury (Ryan et al., 2014). Furthermore, Gabbe et al. (2010) suggested that synergistic and opposing muscle length or ROM can cause an adductor strain. It is speculated that players with a smaller dominant femur diameter are at an increased risk of adductor injuries, as it can alter the origin and insertion points of muscles, consequently altering muscle efficiency, including their ability to generate force and cope with stress (Ryan et al., 2014).
To conclude, there are a variety of modifiable and non-modifiable risk factors for adductor strains. Modifiable factors include strength imbalances, core stability, sport specific training and reduced ROM in hip abduction, while non-modifiable risks include previous injury, level of play, age and femur diameter. In order to prevent adductor strains exercise prescriptions need to be implemented and be based around a client’s health and wellbeing (Eckard et al., 2017).It has been suggested that strength exercises are effective in the prevention of this injury and should consist of progressive resisted adduction and abduction, balance training, core stability training and skating movements on a slide board (Engebretsen et al., 2010).
References
American College of Sports Medicine. (2013). ACSM’s guidelines for exercise testing and prescription. Philadelphia, Pennsylvania: Lippincott Williams & Wilkins.
Biel, A. (2014) Trail guide to the body : How to locate muscles, bones and more (5thed. )Boulder, CO : Books of Discovery.
Buchheit, M., Racinais, S., Bilsborough, J. C., Bourdon, P. C., Voss, S. C., & Hocking, J. (2013). Monitoring fitness, fatigue and running performance during a pre-season training camp in elite football players. Journal of Science and Medicine in Sport, 16(6), 550–555.
Cameron, K. L. (2010). Time for a paradigm in conceptualizing risk factors in sports injury research. Journal of Athletic Training, 45(1), 58–60.
Cowan, S. M., Schache, A. G., Brukner, P., Bennell, K. L., Hodges, P. W., Coburn, P., & Crossley, K. M. (2004). Delayed Onset of Transversus Abdominus in Long-Standing Groin Pain. Medicine and Science in Sports and Exercise, 36(12), 2040–2045.
Eckard, T. G., Padua, D. A., Dompier, T. P., Dalton, S. L., Thorborg, K., Kerr, Z. Y., & Hill, C. (2017). Epidemiology of Hip Flexor and Hip Adductor Strains in National Collegiate Athletic Association Athletes , 2009 / 2010-2014 / 2015. The American Journal of Sports Medicine, 47(12), 2713–2722.
Engebretsen, A. H., Myklebust, G., Holme, I., Engebretsen, L., & Bahr, R. (2010). Intrinsic Risk Factors for Groin Injuries Among Male Soccer Players A Prospective Cohort Study. The American Journal of Sports Medicine, 38(10), 2051–2057.
Esteve, E., Rathleff, M. S., Urrútia, G., & Thorborg, K. (2015). Prevention of groin injuries in sports : a systematic review with meta-analysis of randomised controlled trials. British Journal of Sports Medicine, 49(12), 785–791.
Gabbe, B., Bailey, M., Cook, J., Makdissi, M., Scase, E., Ames, N., & McNeil, J. (2010). Hip and groin injuries in young AFL football players—Pre-existing or a product of the change to the elite senior level? Journal of Science and Medicine in Sport, 12(2), 87.
Johnson, M. E., Mille, M.-L., Martinez, K. M., Crombie, G., & Rogers, M. W. (2004). Age-Related Changes in Hip Abductor and Adductor Joint Torques. Archives of Physical Medicine and Rehabilitation, 85(4), 593–597.
Liu, H., Garrett, W. E., Moorman, C. T., & Yu, B. (2012). Injury rate, mechanism, and risk factors of hamstring strain injuries in sports- A review of the literature. Journal of Sport and Health Science, 1(2), 92–101.
O’Connor, D. M. (2004). Groin injuries in professional rugby league players : a prospective study Groin injuries in professional rugby league players : a prospective study. Journal of Sports Sciences, 22(7), 629–636.
Ryan, J., Mc Creesh, K., & De Burca, N. (2014). Risk Factors for Groin/ Hip Injuries in Field Based Sports: A Systematic Review. British Journal of Sports Medicine,48(14), 1089–1096.
Sathe, P. K. (2017). Assessment and management of adductor strain. Saudi Journal of Sports Medicine, 17(2), 118–120.
Spörri, J., Kröll, J., Amesberger, G., Blake, O. M., & Müller, E. (2012). Perceived key injury risk factors in World Cup alpine ski racing — an explorative qualitative study with expert stakeholders. British Journal of Sports Medicine, 46(15), 1059–1064.
Weir, A., Jansen, J., Keulen, J. Van, Mens, J., Backx, F., & Stam, H. (2010). Short and mid-term results of a comprehensive treatment program for longstanding adductor-related groin pain in athletes : A case series. Physical Therapy in Sport, 11(3), 99–103.
Whittaker, J. L., Small, C., Maffey, L., & Emery, C. A. (2015). Risk factors for groin injury in sport : an updated systematic review. British Journal of Sports Medicine,49(12), 803–809.
Zaleski, A. L., Taylor, B. A., Panza, G. A., Wu, Y., Linda, S., Thompson, P. D., & Fernandez, A. B. (2016). Coming of age : Considerations in the prescription of exercise for older adults. Methodist DeBakey Cardiovascular Journal, 12(2), 98–104.