Running total of hours: 103.5
Patient 1 – Patient Overview: regular weekly or fortnightly STM. Noticeable improvements in range of motion of neck and shoulders with a decrease in pain when putting on her coat. The progress in these sessions have been incredibly slow due to my inability to fully perform the treatment that may be most effective for the patient; mobilisations of the neck. This is due to the patient’s inability or discomfort in the thought of lying on the treatment couch and as such all STM is performed while the patient is sitting on the couch with legs over the side. The patient is happy with progress, knows the limitations in STM but reports positivity and provides good feedback for each session and wishes to continue the STM sessions on a weekly basis to supplement her physiotherapy appointments in between.
Patient 2 – Metatarsalgia follow up – No improvements but has recently developed new pain in lateral ankle, inferior to lateral malleolus over peroneal tendons. This has stopped the patient from running and fully engaging in rehabilitation and strengthening exercises.
According to findings by Männikkö & Sahlman (2017), orthotic inserts in the form of padding placed inside the shoes was effective as a treatment intervention to reduce pain and improve the scores of a questionnaire designed to evaluate lower limb pathology and has been reported as being one of the most commonly used foot scores for lower limb; The American Orthopaedic Foot & Ankle Society Forefoot Questionnaire (AOFAS). It must be noted however that although questionnaires in similar forms, such as the Self-Reported Foot and Ankle Score (SEFAS) and the Foot and Ankle Score (FAOS) have been found to be effective in correctly evaluating the presence of or change in dysfunction or injury presentation in the lower limb, the sheer range of foot disorders limits the ability to target certain pathologies which present with more specific symptoms. Although the AOFAS is a reliable measure, for future reference within a clinical setting, a questionnaire similar to the SEFAS may be a more useful tool as not only was it found to be a reliable and a feasible patient-reported outcome measure, it was also reported as being a much more user friendly method due to the time taken to complete; the AOFAS requires four comprehensive and resource demanding questionnaires, whereas the SEFAS requires scores on just pain, function and functional limitations but still maintained its reliability (Cöster et al., 2014).
Metatarsalgia can be the result of a number of risk factors, such as mechanical predisposed conditions such as pes planus, hammer toe, hallux valgus or hypermobility in the metatarsal joints and can be brought on by increased loading, fat pad alignment, but most interestingly rheumatoid arthritis (Männikkö & Sahlman, 2017). This patient is currently undergoing testing for Rheumatoid Arthritis after an appointment with his GP, due to a family history of the condition and the symptoms in his foot; it will be interesting to find out the results of this and how and if this may affect treatment. In the meantime, the use of padding or inserts are a good way to redistribute landing forces during walking or running and as such, this was given to the patient. A number of other studies including one by Besse (2016) have recommended the use of padding over the head of the metatarsal in order to create a new point in which the pressure is loaded upon and landing forces are dispersed over a larger surface area.
In order to fully test the effectiveness of this treatment, we did not change any other variables and kept his exercise program the same, as given at the previous session; if the patient reports a reduction in pain by the next session, then we can associate this with the padding and if there is no change, we can add another variable.
Figure 1 is of the typical location of metatarsalgia and is an accurate representation of where this patient felt most discomfort and pain and Figure 2 demonstrates when in the shoe the padding was placed.
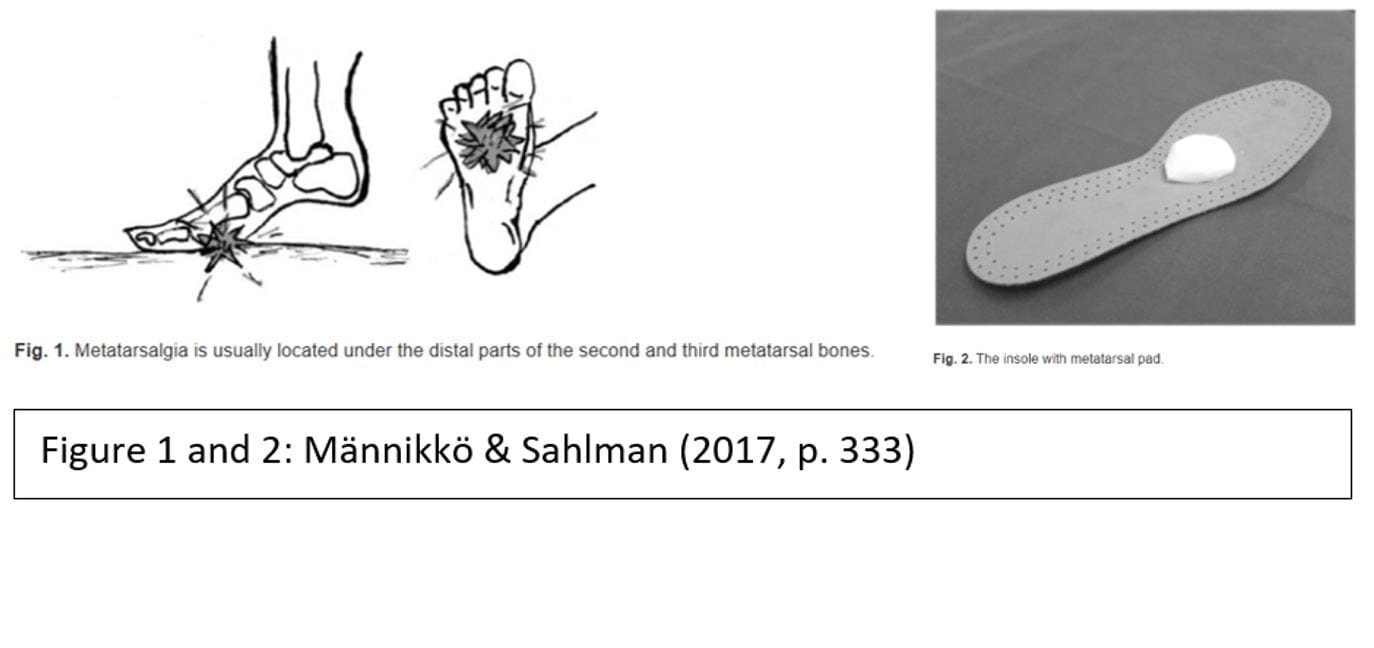
Although this method has been found to be of clinical use, it has also been found that a general insole with whole forefoot cushioning is effective in reducing and dispersing landing forces and peek pressure in the forefoot and is recommended over the more specifically located metatarsalgia padding as shown in Figure 2 (Hähni, Hirschmüller and Baur, 2016).
Because we did not have any orthotic inserts in the clinic to offer the patient, we constructed our own version of the padding shown in Figure 2.
If the patient reports some improvement with the extra padding, then we are able to better understand the mechanics of his injury. If there are no improvements, I can suggest the use of a more evenly constructed orthosis for our next option, such as the one used in a study by Hähni et al. (2016) as it eliminates patient application error and movement of the padding during activity; the location consistency may be compromised (Männikkö & Sahlman, 2017). The use of an orthosis may also provide enhanced positive effects in comparison to the padding, as shown by Hähni et al. (2016).
Patient 3 – STM treatment of the triceps surae group for the treatment of reduced dorsiflexion and pain in calf muscle.
This patient presented with significant feeling of “tightness” and associated pain of the triceps surae muscle group, more specifically the soleus (this was deduced through the isolation of the soleus muscle in a tandem stance lunge style stretch whereby the posterior leg being stretched is bent, eliminating the gastrocnemius muscle when the knee is flexed as this crossed over both the posterior knee onto the femur and the ankle via the calcaneal tendon).
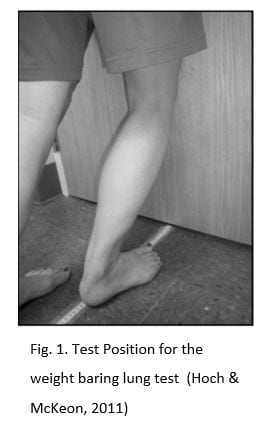
As mentioned in a previous post, the knee to wall test, also known as the lung test, is a useful measure for ankle dorsiflexion; it is a good indicator of muscle or joint restriction when compared with the contra lateral leg, or an indicator of improvements after treatments. It is commonly reported that tightness in the triceps surae group can cause a reduction in ankle dorsiflexion, which is a contributing factor in the future risk of injury (Hoch & McKeon, 2011).
When I performed this test in the clinic, I was not sure about the measurements that were of significance. According to Hoch & McKeon (2011), asymmetry can be determined by a difference of >1.5cm between each ankle. In this case, asymmetry was not present as the patient presented with bilateral tightness and subsequent restrictions in ankle dorsiflexion in both ankles.
In order to help reduce risk of future ankle injury and reduce pain and tightness, I administered treatment to lengthen the triceps surae muscles by way of soft tissue massage, stretching, exercises and derived a take home plan to maintain these treatment effects, which also involved self-administered soft tissue massage such as foam rolling (Wiewelhove et al., 2019).
Soft tissue therapy is widely used in the treatment of soft tissue injuries, but the efficacy of its use is also often disputed. There is a great body of evidence to disregard the effectiveness of this modality, however conversely there are also findings proving its effectiveness; the use of soft tissue massage should therefore be advocated only on a case by case basis and measures to test it’s effectiveness put in place.
According to findings by Thomson, Gupta, Arundell and Crosbie (2015), deep soft tissue massage is not an effective treatment for muscle stiffness or restricted ankle dorsiflexion; no significant differences in extensibility or reduced stiffness was found. This study was conducted using a reportedly highly reliable test method but only included 29 healthy subjects without any musculoskeletal injury. Although this study found massage as ineffective on a small sample of healthy subjects, these findings may not be representative of the wider population and research needs to be done on the effects on injured or dysfunctional tissue. Early research by McKechnie, Young and Behm (2007) on the effectiveness of two different massage techniques found that just three minutes of massage by tapotement or petrissage over the muscles that plantarflex the ankle (peroneal longus and brevis, gastrocnemius and soleus) improved ankle flexibility, but not with an associated reduction in power, justifying the use of this modality for at least a short term treatment option. Interestingly, no differences were found between the two types of massage, therefore an application for either can be effective.
In a study on 50 female hockey players, dynamic soft tissue massage was compared to regular massage in the treatment of increasing hamstring length with both control and intervention group experiencing increases after treatment, suggesting the benefits of massage in general on increasing tissue length in muscles (Hopper et al., 2005).
More recent research on a larger sample size of 60 subjects by Stefansson, Brandsson, Langberg and Arnason (2019) for example, found that pressure point massage was effective in the treatment of Achillies Tendinopathy, an injury presenting with muscular tightness in the triceps surae group as a risk factor. The positive effects of pressure massage, therefore could imply that mechanical effects do occur as a result of STM, as previously refuted by Thomson et al. (2015).
Although there is conflicting evidence and varying recommendations on the effectiveness and efficacy of STM for exercise recovery, ROM, exercise performance and stiffness, the use of STM for the reduction of pain has been reported and evidenced in studies such as a study by Romanowski et al. (2012), showing that massage, both therapeutic and deep tissue can have positive effects on pain in individuals with chronic lower back pain and Kumar, Beaton and Hughes (2013) who found that massage produced short term pain reduction in chronic lower back pain.
Interestingly, in a review on the effects of STM by Piper et al. (2016), soft tissue therapy was found to be effective in some injuries, such as lateral epicondylitis and plantar heel pain, however it was highlighted that movement education was also effective in treating lateral epicondylitis, implying neuromuscular adaptations. This posed the question of whether any reported effects of massage is correlated to the physiological changes in the soft tissue, or the neuromuscular interpretation of muscular length, with reports published on the effects on neurological effects of massage (Sefton, Yarar, Carpenter and Berry, 2011).
Other factors in the reduction of pain can be discussed, such as the combination of physiological and psychological effects.
It has been reported that massage can have a variety of other benefits as well as the reduction of pain, including improvements in stress levels, emotional wellbeing and physical recovery; found in a study by Adams, White and Beckett (2010) when administered in the early stages of their treatment or care in a hospital setting.
Figure 1 shows the test procedure of the test used as an objective marker (Hoch & McKeon, 2011). Not only was I able to confirm the physiological adaptations and effectiveness of the massage treatment by way of qualitative feedback of reduced pain from the patient, but the patient was able to see for herself the effectiveness of the session, hopefully providing her with motivation to maintain a home program outside of the clinic setting.
I will ask the patient to perform the test again in her next session, as this may be a suitable indicator of exercise and stretching adherence over the coming weeks.
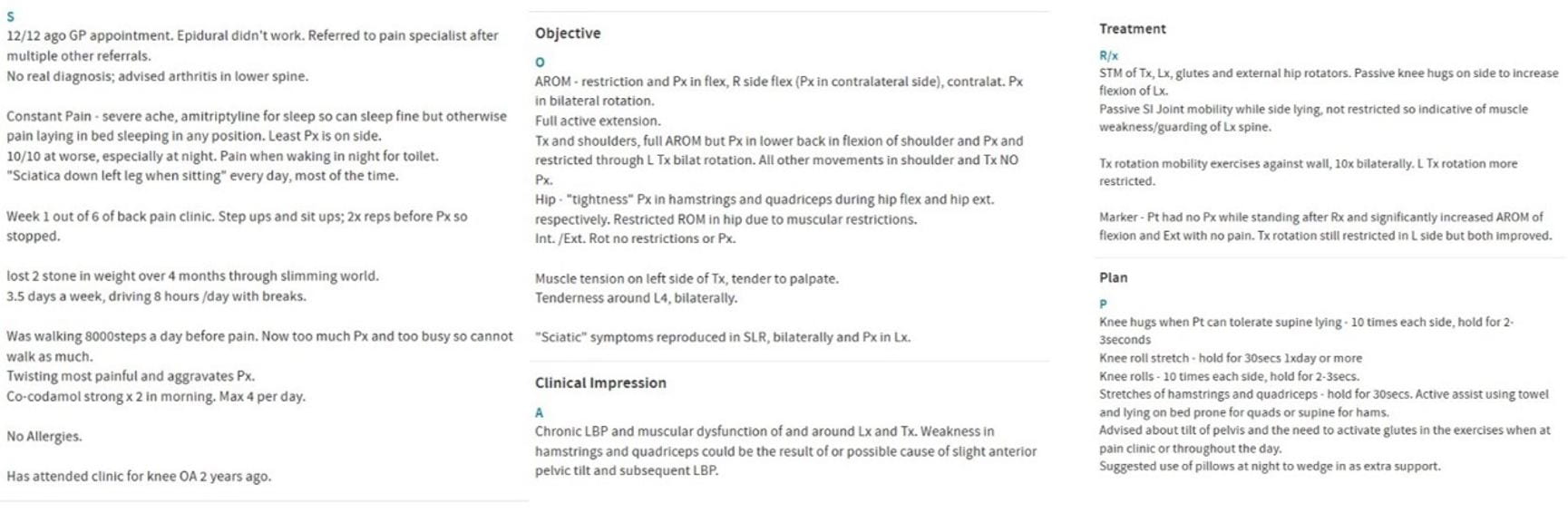
Patient 4 – STM of lower back
Patient Overview – This patient is very physically active, attending the gym most days. He presented with chronic lower back pain which is being managed and treated by a variety of care providers including the sports therapy clinic at Marjon. The patient has already been assessed and asked specifically for a soft tissue massage only as a means to compliment the stretching and exercise program he was prescribed at his previous treatment sessions.
Non-specific Low Back Pain (NSLBP) has a prevalence of up to 33% and accounts for 85-90% of lower back pain (Kachanathu et al. (2014). Although most individuals with lower back pain respond well to treatment in the early stages, according to Kachanathu et al. (2014) up to 15% end up with a chronic condition.
As the patient has felt improvements and positive effects of soft tissue massage for his lower back, he was satisfied with the nature of the treatment. I made sure to ask for feedback throughout the treatment, ensuring that I was applying the desired pressure.
I checked the patients ROM and updated his records to reflect this so that improvements can be made and used pain and patient reported stiffness as marker for improvement and performed deep tissue massage and myofascial release to his whole lower back and thoracic spine as well as deep tissue massage through his glutes and external rotators. Deep tissue massage has been reported as more effective than therapeutic massage in the treatment of lower back pain, so I needed to ensure I was applying the appropriate pressure. I mobilised his lower spine using posterior anterior grade IV oscillations to help reduce pain and increase ROM in lumbar extension and flexion, as found effective in the treatment of NSLBP (Shah & Kage, 2016).
In order to help the patient to improve his LBP on a more long term time scale, mobility exercises such as the cat camel, knee rolls, knee hugs and strengthening of the abdominal and gluteus muscles were given and stretching of the hip flexors, hamstrings and back were advised as recommended by a study finding the positive outcome of this treatment in patients with chronic LBP (Kachanathu et al., 2014).
Extra hour between patients – I spend this hour trying to increase my dorsiflexion range of motion through a range of interventions; mobilisations with movement using a resistance band and by performing squats. I practiced performing the knee to wall test and found noticeable improvements using both methods. I am aware of my dorsiflexion restriction, particularly in my right ankle due to previous lateral ankle sprain injuries and so I knew that joint mobilisations would be more effective than general soft tissue massage of the trceps surae group alone.
From this practice, I was able to fully appreciate the need for the non tested foot to have the heel flat on the floor so as to no wrongly add further range to the tested ankle. Trying out these tests and exercises myself is a good way to understand them in a better way in order for me to demonstrate them better and more efficiently to my patients in future.
References –
Adams, R., White, B., & Beckett, C. (2010). The effects of massage therapy on pain management in the acute care setting. International Journal of Therapeutic Massage and Bodywork: Research, Education, and Practice, 3(1), 4–11. https://doi.org/10.3822/ijtmb.v3i1.54
Besse, J.-L. (2016). Review article Metatarsalgia. 103, 29–39. https://doi.org/10.1016/j.otsr.2016.06.020
Cöster, M. C., Bremander, A., Rosengren, B. E., Magnusson, H., Carlsson, Å., & Karlsson, M. K. (2014). Validity, reliability, and responsiveness of the Self-reported Foot and Ankle Score (SEFAS) in forefoot, hindfoot, and ankle disorders. Acta Orthopaedica. https://doi.org/10.3109/17453674.2014.889979
Hähni, M., Hirschmüller, A., & Baur, H. (2016). The effect of foot orthoses with forefoot cushioning or metatarsal pad on forefoot peak plantar pressure in running. Journal of Foot and Ankle Research, 9(1), 7–13. https://doi.org/10.1186/s13047-016-0176-z
Hoch, M. C., & McKeon, P. O. (2011). Normative range of weight-bearing lunge test performance asymmetry in healthy adults. Manual Therapy, 16(5), 516–519. https://doi.org/10.1016/j.math.2011.02.012
Hopper, D., Conneely, M., Chromiak, F., Canini, E., Berggren, J., & Briffa, K. (2005). Evaluation of the effect of two massage techniques on hamstring muscle length in competitive female hockey players. Physical Therapy in Sport, 6(3), 137–145. https://doi.org/10.1016/j.ptsp.2005.04.003
Kachanathu, S. J., Alenazi, A. M., Seif, H. E., Hafez, A. R., & Alroumim, A. M. (2014). Comparison between Kinesio taping and a traditional physical therapy program in treatment of nonspecific low back pain. Journal of Physical Therapy Science, 26(8), 1185–1188. https://doi.org/10.1589/jpts.26.1185
Kumar, S., Beaton, K., & Hughes, T. (2013). The effectiveness of massage therapy for the treatment of nonspecific low back pain: A systematic review of systematic reviews. International Journal of General Medicine. https://doi.org/10.2147/IJGM.S50243
Männikkö, K., & Sahlman, J. (2017). The Effect of Metatarsal Padding on Pain and Functional Ability in Metatarsalgia. Scandinavian Journal of Surgery. https://doi.org/10.1177/1457496916683090
McKechnie, G. J. B., Young, W. B., & Behm, D. G. (2007). Acute effects of two massage techniques on ankle joint flexibility and power of the plantar flexors. Journal of Sports Science and Medicine, 6(4), 498–504.
Piper, S., Shearer, H. M., Côté, P., Wong, J. J., Yu, H., Varatharajan, S., … Taylor-Vaisey, A. L. (2016). The effectiveness of soft-tissue therapy for the management of musculoskeletal disorders and injuries of the upper and lower extremities: A systematic review by the Ontario Protocol for Traffic Injury management (OPTIMa) collaboration. Manual Therapy, 21, 18–34. https://doi.org/10.1016/j.math.2015.08.011
Sefton, J. E. M., Yarar, C., Carpenter, D. M., & Berry, J. W. (2011). Physiological and clinical changes after therapeutic massage of the neck and shoulders. Manual Therapy. https://doi.org/10.1016/j.math.2011.04.002
Shah, S. G., & Kage, V. (2016). Effect of seven sessions of posterior-to-anterior spinal mobilisation versus prone press-ups in non-specific low back pain-randomized clinical trial. Journal of Clinical and Diagnostic Research, 10(3), 10–13. https://doi.org/10.7860/JCDR/2016/15898.7485
Stefansson, S. H., Brandsson, S., Langberg, H., & Arnason, A. (2019). Using Pressure Massage for Achilles Tendinopathy: A Single-Blind, Randomized Controlled Trial Comparing a Novel Treatment Versus an Eccentric Exercise Protocol. Orthopaedic Journal of Sports Medicine, 7(3), 1–10. https://doi.org/10.1177/2325967119834284
Thomson, D., Gupta, A., Arundell, J., & Crosbie, J. (2015). Deep soft-tissue massage applied to healthy calf muscle has no effect on passive mechanical properties: A randomized, single-blind, cross-over study. BMC Sports Science, Medicine and Rehabilitation, 7(1), 1–8. https://doi.org/10.1186/s13102-015-0015-8
Wiewelhove, T., Döweling, A., Schneider, C., Hottenrott, L., Meyer, T., Kellmann, M., … Ferrauti, A. (2019). A meta-analysis of the effects of foam rolling on performance and recovery. Frontiers in Physiology. https://doi.org/10.3389/fphys.2019.00376