
Date: 16.01.2020
Duration: 0900 – 1030 – 1.5 hours
Venue: Marjon Sports Therapy Clinic
Reflective Summary:
My client was a very active individual participating in rowing, sitting volleyball, shotput, discus, swimming and wheelchair rugby events for the Invictus Games. She also regularly plays netball, basketball, swimming and waterpolo. She is active every day. She is a mother of two children under five and two adults over twenty years-old. She is also studying on a sports rehabilitation degree and revising for upcoming exams.
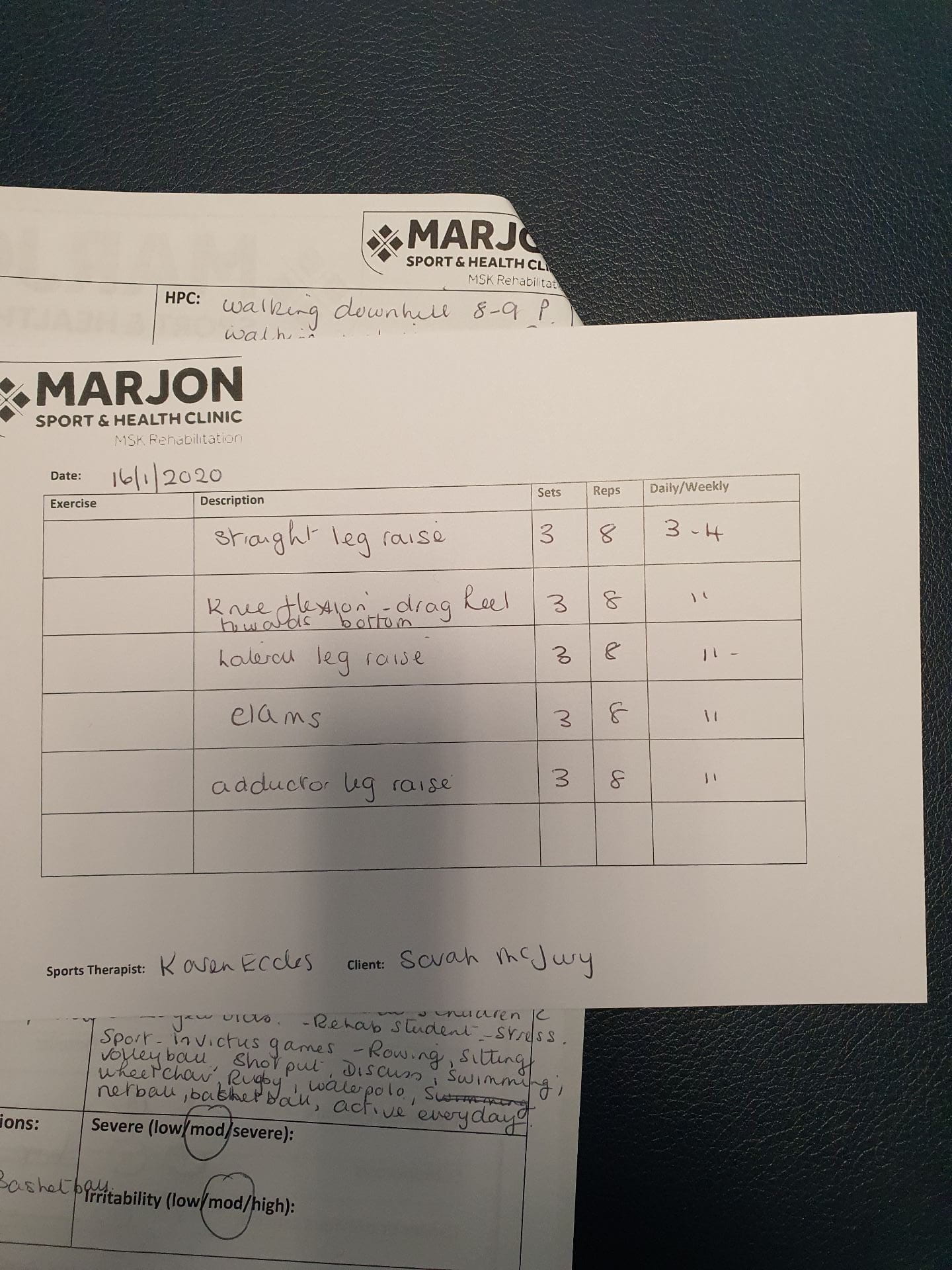
She fell off of a curb on 5.12.19 directly onto her knee. She finds it pain walking downhill NRS levels 8-9, walking uphill levels4-5 and walking upstairs level 5. She is still unable to bare weight on the knee. Recently she started playing basketball after a rest after being unwell and it has aggravated her injury further.
After the subjective assessment I had a pretty clear idea that the injury was either Meniscus damage or possible ACL.
In the objective assessment during palpation my impression was still meniscus damage but instead of an ACL injury, my thoughts were leading to MCL because there was some inflammation on the medial side of the knee and there was a high pain level (L9) after palpation of the medial and lateral epicondyles. There was also tenderness above the knee around the quads and underneath the patella.
There was a lot of pain in knee flexion around 40-50 degrees both in AROM and PROM. Reduced strength in FL and internal rotation.
I ruled out the ACL and MCL ligaments with negative anterior draw and valgus stress tests. I also checked the ITB – but the Nobles test was a false positive.
Meniscus damage was confirmed by a positive Thessaly’s, Apley stress test with compression. Medial meniscus tear was confirmed with a positive McMurray test with the tibia externally rotated.
I prescribed a programme of active exercises to improve strength in all of the surrounding muscles and once the client felt stronger, advised her to progress onto performing the exercises with a theraband. She could also cycle on a static bike and swim, but avoid too much or too little resistance on the bike and swim strokes that aggravated the knee. She could swim with a pool bouy until the knee felt stronger.
I felt positive and confident throughout the examination and performed a k-taping around the knee to provide support.
Areas for further improvement plus action plan
Review K-taping techniques