March 2022 – June 2022
Hours: 12
Patient decided to continue with rehabilitation and completed a further 12 hours at 2 x 45 minutes session per week.
Patient presentation:
- 10 year old girl with right hemiplegia
- She has a leg length discrepancy due to excessive tone in her calves which causes tip-toe walking.
- Parents want to focus on stretching the calf complex, strengthening the right lower limb and increasing adherence to exercises.
- The patient wants to improve core and upper limb strength.
- Her right upper limb is weak – she has poor grip strength and inhibited motor skills
The upper limb in currently not a focus at the patient has had botox and all stakeholders want to capitalise on its effects.The upper limb in now something they wish to focus on.- After a meeting with their consultant they would like to be more ‘aggressive’ with exercising her affected side.
Reflection Model
- Gibbs Reflective Cycle 1988
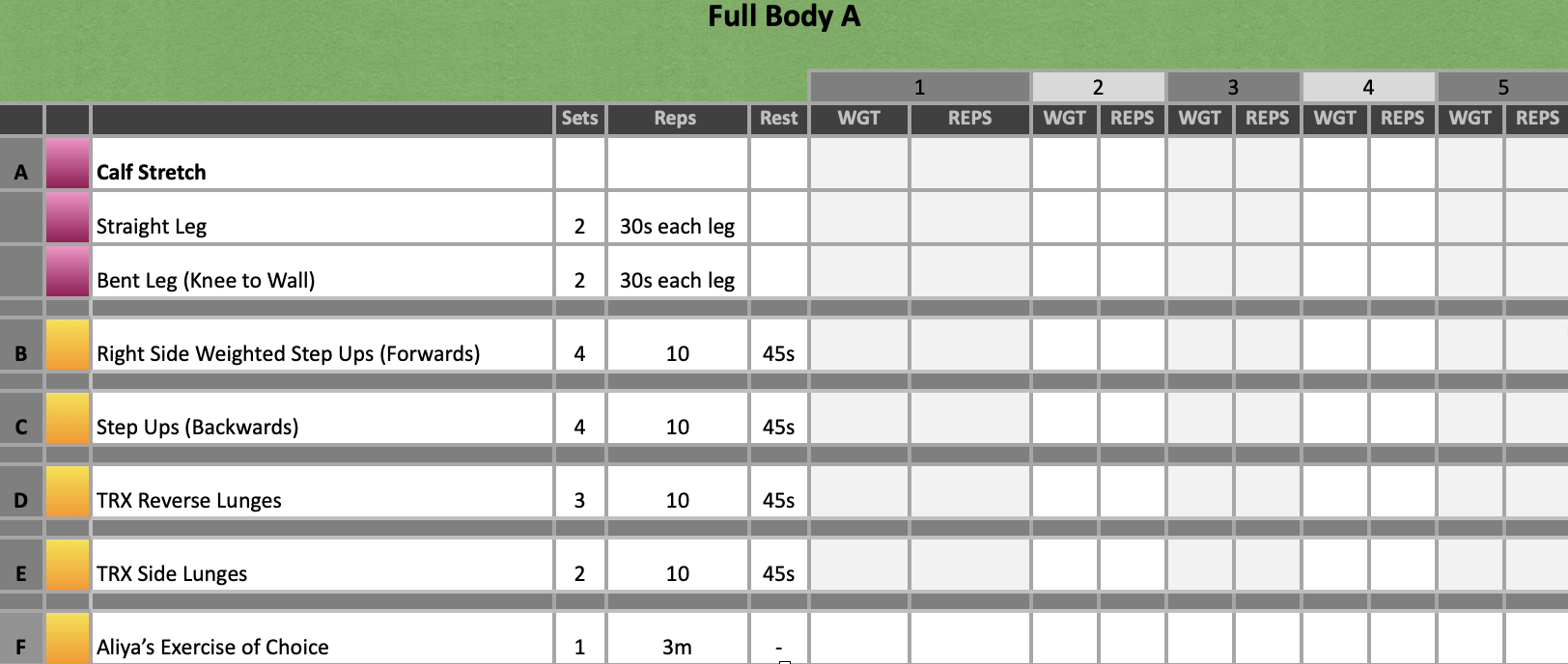
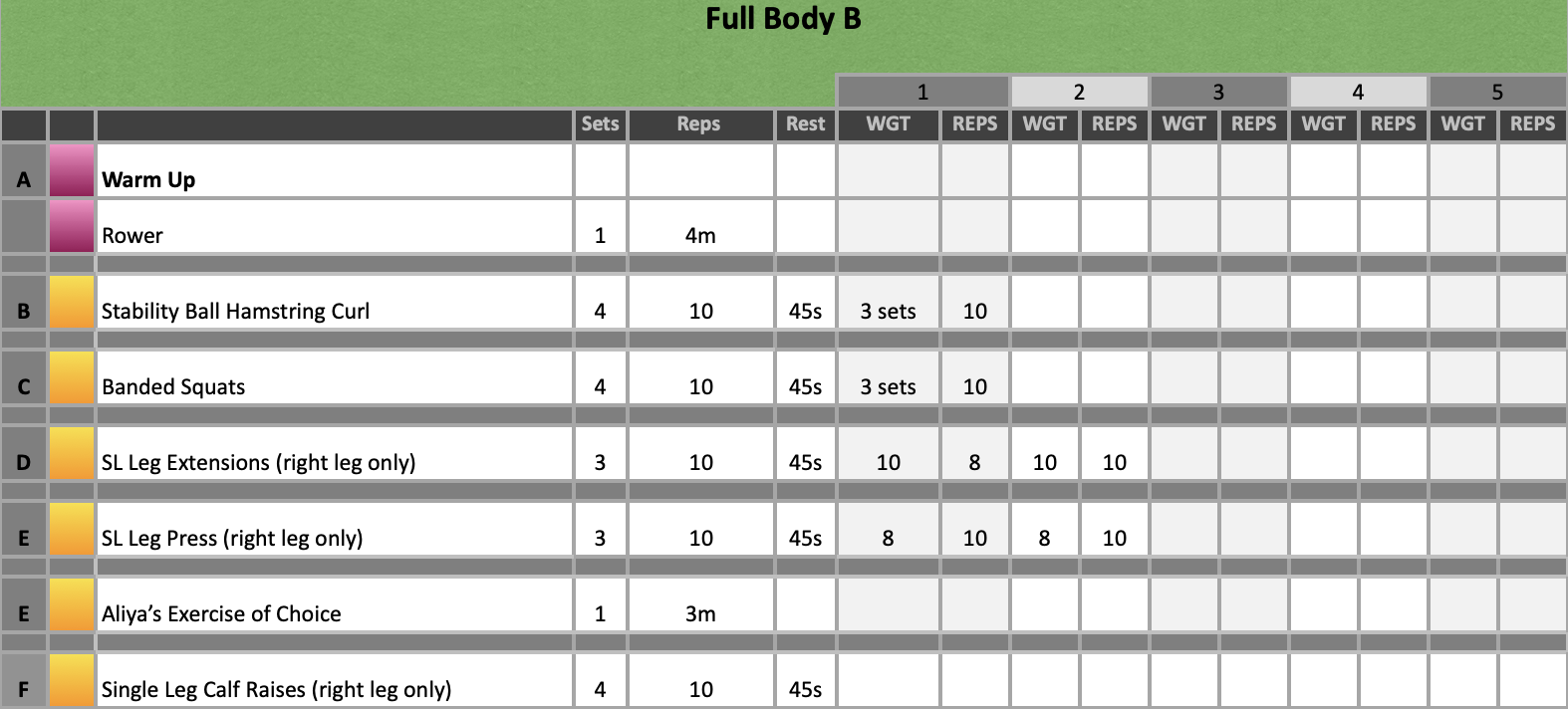
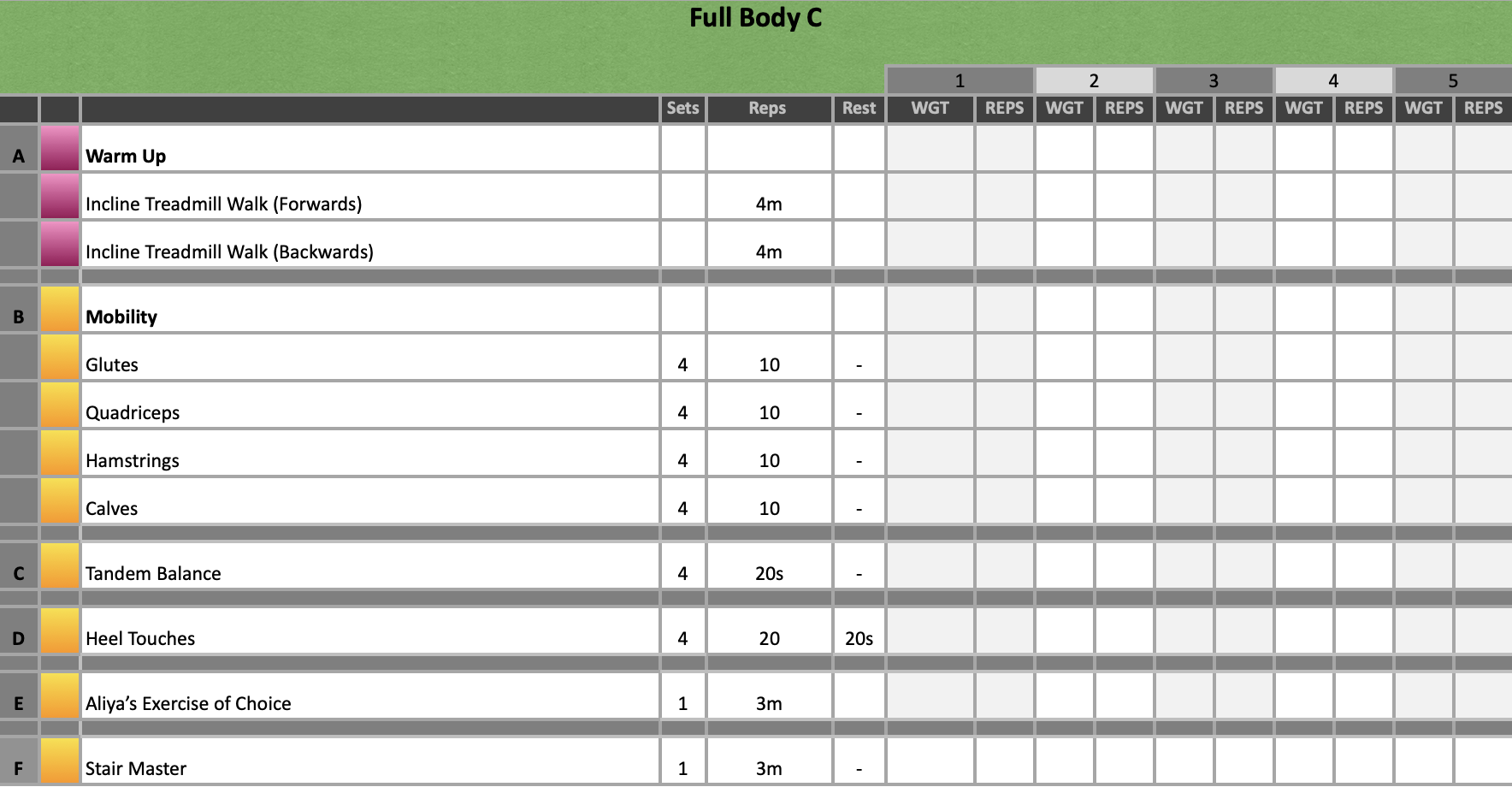
Exercise Prescription
What Happened?
- After meeting with the patients consultant, I was asked by the parents to focus entirely on her right leg during training sessions.
- The patient also wanted to improve her upper body strength so we incorporated that into her exercises of choice.
- We continued to progress steps ups as highlighted before. We also incorporated balance work into step ups from time to time too.
- Core work was added in the form of heel touches; however, we varied this and completed kneeling pallof presses, hanging knee/leg raises and partner assisted leg pushes.
What were you thinking and feeling?
- Training just one side seemed to go against what I believed to be an important principle of rehab – treat both sides. However, in cases like this there is evidence that immobilising the more functional side of the body, thus forcing the affected side to work can have better outcomes for patients with hemiplegia. Further to this, we were actually able to get more done in the sessions as we were only focusing on one side.
- I have started implementing external forces such as resistance bands to correct knee valgus during squats as I want to ensure that the movement is encouraging optimal biomechanics. We have also started to focus on foot placement of the affected side which is difficult for the patient; however, this is once again to encourage optimal alignment and movement patterns.
Analysis and Evaluation
- The patient’s balance is consistently improving – she can now intermittently balance on her affect side when performing step ups. Both the patient and her parents were elated with this which was so lovely to see.
- The patient is also starting to become more confident in the gym setting and less self-conscious of her affected side. Previously, she would always try to hide taking her splint on and off and she would also always choose to start exercises on her left. This could have potentially been out of habit but as time has progressed she knows that it is the right side she needs to use so she is picking up weights with that side more often now.
- We have to change SL leg press as the patient really didn’t like the exercise. We substituted it for single leg supported half squats which she found much more manageable.
Conclusion
- The patient has done well with the introduction on single leg work only and her strength has increased quite significantly in this block compared to the previous. This is likely due to the extra volume we can get through her affected side and shows that currently there are no adverse effects training in this way for her.
- I am starting to run out of creative exercises for the patient and I am concerned she may get bored if we keep things the same for too long – equally this could result in a plateau so I need to look into developing the current exercises further whilst maintaining the patients enjoyment so she will continue with her training.
References
- Baechle, T. R., Earle, R. W., & National Strength & Conditioning Association (U.S.). (2008). Essentials of strength training and conditioning. Champaign, IL: Human Kinetics
- Das, S. P., & Ganesh, G. S. (2019). Evidence-based Approach to Physical Therapy in Cerebral Palsy. Indian journal of orthopaedics, 53(1), 20–34. https://doi.org/10.4103/ortho.IJOrtho_241_17
- Gbonjubola YT, Muhammad DG, & Elisha AT. (2021). Physiotherapy management of children with cerebral palsy. Adesh Univ J Med Sci Res 3, 64-8.