10th January – 16th January
- Hours: 15
Main Theme Addressed During Phone Calls
- Thoughts, feelings and questions from week 7’s gym drop-in.
- Discussing specific exercises that may benefit particular individuals
- For example, calf raises for marathon runner and patient suffering from proximal fatigue.
- One patient, who has never, used the gym before was really lacking confidence and wasn’t sure if she would come again this week.
- All participants who attended the gym and/or class in person noted a real difference in motivation and enjoyment.
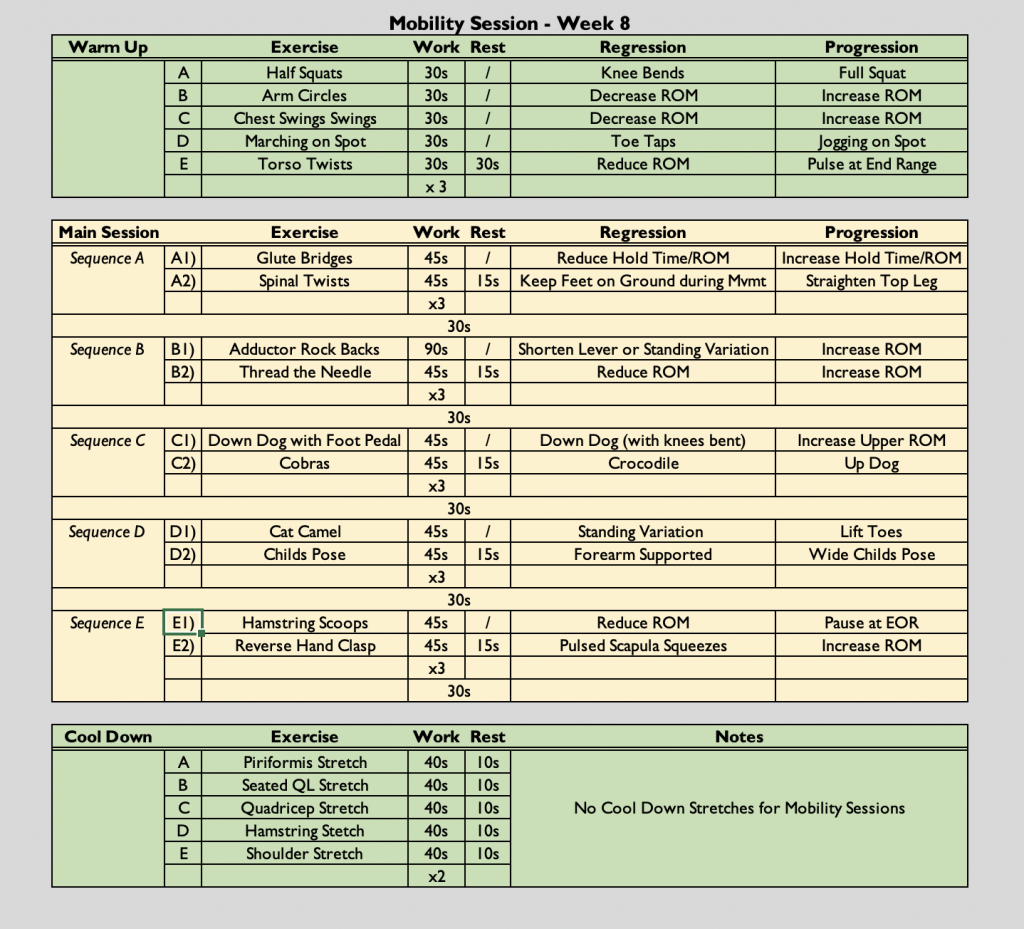
Mobility Class
- ((45s secs x 2 followed by a 30 second rest) x 3) x 3
- The class is always symptom-led as opposed to graded exercise therapy. Participants are free to rest when needed. They can end the class early if they have reached their limit and they can reduce the amount of sets they do if necessary.
Gym Drop-In Session
- The participant who was lacking confidence joined me as I delivered another gym induction for a participant who couldn’t attend the week previously. She printed off the gym programme I provided during week 7 to carry around with her. After trying a couple pieces of equipment things started to click into place and she stated that she understood everything a bit more so felt more confident. I had to leave her and the individual who hadn’t completed the gym induction previously to help some of the other participants during the drop-in. When I came back she was mid-way through demonstrating how the leg extension worked to her fellow participant. After this the participant seemed to have found some confidence and happily approached some more equipment without needing my direct support.
Analysis & Evaluation
- I was really keen to individualise programmes as best as possible for patients – not only to address specific concerns individuals may have e.g. knee pain, but also to keep the gym sessions relevant to their recovery goals. For example, the marathon runner would like to get back to running so I wanted to show him some strength and conditioning he could do to support his return to running e.g. calf raises. My aim here was to hopefully keep the individuals motivated to attend gym sessions as it is relevant to what they are looking to achieve from the programme. This was also the week that this participant introduced run/walk into his exercise routine – he completed 1km using a run/walk strategy. He noted that he was a bit more breathless and wheezy than he expected but he forgot to take his inhaler (asthmatic) prior, which he used to always do. Therefore, I encouraged him to try again next week with the inhaler to see if that makes his breathing easier.
- The participants noted that it was really nice and enjoyable to meet everyone in person and it lifted their spirits. This highlights that the virtual/telerehabilitation component of the programme, although beneficial for most, maybe wasn’t as enjoyable as the face-to-face component of the programme. Many noted that even though you are in a group setting during the virtual phase you feel like you are going it alone still but when you meet everyone in person you feel like you have more of a support network and a chance to form meaningful bonds with others who need your help and support too. This highlights both the benefits and drawbacks to telerehabilitation and potentially also group v individual rehabilitation. For example, telerehabilitation can be completed successfully in the convenience of your own home; however, it lacks the same social experience as face-to-face that people quite often prefer. Furthermore, group rehabilitation can provide a wider support network that might not be as easily accessible as individual rehabilitation. However, group rehabilitation can make it slighter harder for the therapist to individualise parts of the session. This is why I spend time working with individuals during the drop-in session as it is a chance to tackle the drawback of group rehabilitation.
Conclusion
- From the feedback this week, I am going to explore ways in which to boost motivation and morale during the telerehabilitation stage of the programme.
- Psychosocial support is a key component of rehabilitation (Wade. 2020). There are many techniques that can be used to provide this support, such as rehabilitation in a group setting. I enjoy working with participants on a one to one basis; however, this experience and literature has highlighted that group rehabilitation is a useful strategy for helping individuals with their psychosocial needs. I feel this is particularly true of COVID-19 rehabilitation as nation wide lockdowns resulted in a significant lack of social interaction with friends and family – a key component to maintaining healthy emotional wellbeing.
Revisiting Reflection
References
- Wade D. T. (2020). Rehabilitation after COVID-19: an evidence-based approach. Clinical medicine (London, England), 20(4), 359–365. https://doi.org/10.7861/clinmed.2020-0353