Monday 14th March 2022
Hours: 3
Patient presentations:
- Netball player with suspected WAD
- Football player – lateral ankle sprain
Reflection Focus
- Suspected WAD – Grade 2
Reflection Model
- Gibbs Reflective Cycle 1988
What Happened?
- Patient’s 2nd visit to clinic – I observed her first visit whilst she was treated by another therapist.
- Patient fell during a game of netball and fell backwards. She was unsure if the back on her neck hit the opposing player first of if she hit the ground first.
- Reporting pain and tightness during flexion and extension – extension is particularly painful. After the initial injury she was taken off the field of play and concussion was ruled out by a therapist on site.
- Pain leads up to the occiput and the patient is also complaining of tightness in UFT.
- Reported headaches and dizziness after the trauma but this dissipated within 2 days
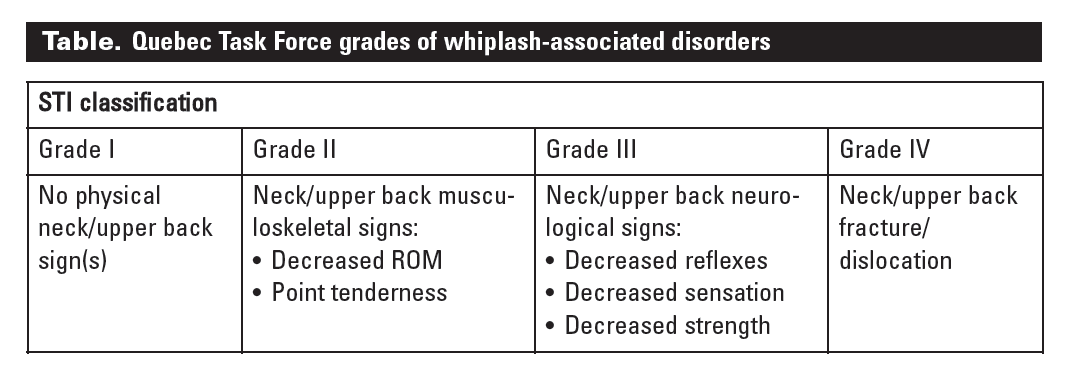
- Patient is now 3 weeks post-trauma – according to the Quebec Task Force classification system the patient fits into the grade 2 classification. As she has decreased ROM and can pin point an area of tenderness on her neck.
- Treatment was STM and MET to relieve UFT tightness – effleurage and petrissage. Pt reported slight improvement in regards ride sided tightness.
- MET of UFT – pt experienced a painful tightness.
- Pin and stretch technique not tolerated due to pain.
- Exercises – Chin tucks against gravity and chin tucks with flexion.
- Discussed DSE as patient reported that sitting for long periods at her desk aggravate symptoms.
What were you thinking and feeling?
- This is the first time in clinic I can say that I genuinely felt tightness in a muscle compared to the muscle on the opposite side. The patients R UFT had obvious and palpable increased tone/tension. The treatment I offered seemed mildly effective. Other treatments that I thought would be beneficial; however, could not be tolerated due to pain. This was frustrating, I am sure for the patient also, but I didn’t want to invoke too much pain that it promoted further guarding.
Analysis and Evaluation
- I remembering being taught about whiplash but I couldn’t really remember anything in regards to treatment. In this instance I just applied the basics of rehabilitation – I identified the patients main complaint and treated accordingly. A systematic review in 2012, found that evidence for treating grade 2 WAD is limited and of low quality; however, active interventions seemed to be more favourable for patient outcomes (Rushton, et al., 2011). Therefore, it is possible that the prescriptive exercises may yield improvements – the patient did report that symptoms had improved since her first visit and she had been keeping up with her exercise prescription.
Conclusion
- I think I still have a lot of work to do in regards to acquiring the knowledge and skills to treat WAD. The literature I found on this seemed dated and so I wonder if this resulted in academics publishing more high quality evidence for this pathology.
- I am going to do some further reading before I next see the patient (March 24th) to ascertain how I could change the treatment plan in order for relive her pain and discomfort.
Revisiting Reflection
References
- Rushton, A.B., Wright, C.C., Heneghan, N.R., Eveleigh, G., Calvert, M.J., & Freemantle, N. (2011). Physiotherapy rehabilitation for whiplash associated disorder II: a systematic review and meta-analysis of randomised controlled trials. BMJ Open, 1.