Monday 23rd August 2021
Hours: 5
Patient presentations:
- Knee pain post-trauma
- Shoulder pain localised to greater tuberosity
- Lateral Ankle Sprain
Reflection Focus
- Shoulder Pain Localised to Greater Tuberosity
Reflection Model
- Gibbs Reflective Cycle 1988
What Happened?
- I had treated this patient previously.
- The patient’s pain was sporadic. Some days the pain wouldn’t bother her and other days it would feel as though she was ‘back to square one.’
- The stretches that were prescribed provided relief in the moment but were clearly not a permanent solution to her pain.
- On reassessing her ROM she was pinpointing the painful/restricted area to approx. greater tubercle of the humerus. This raised my index of suspicion for a rotator cuff injury due to where the rotator cuff muscle group insert.
- The patient mentioned during this session that she participates in dinghy racing from April to September. The patient stated that this sport involves pulling rope towards her and keeping tension on it for a significant period of time when training and racing.
What were you thinking and feeling?
- When the patient mentioned that she participated in dinghy racing I knew I had made a mistake during my previous assessment. I had failed to take a thorough subjective history and as a result, I missed an important factor that could have been contributing to the patient’s pain. As frustrating as it was to know that I had made such an obvious mistake I was relieved that I had more information that I could use in order to support the patient.
What was good and bad about the experience? & Analysis
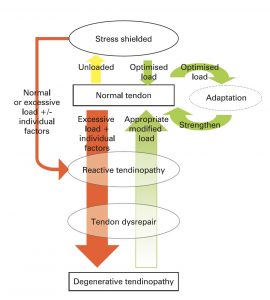
- To have a more complete picture of the patient and her injury was extremely useful. I was able to ask further questions about dinghy racing and it turned out that she doesn’t complete any form of training in the ‘off-season.’ This once again raised my index of suspicion for an overuse injury as she had gone from doing very little sport-specific activities to training and racing at least once a week. This allowed me to provide some education to the patient about the importance of gradually increasing her training activity. Based on Cook and Purdam’s Tendinopathy Pathology Continuum (2009), I explained that overuse injuries tend to occur when the body is exposed to too much load, too often and doesn’t have enough time to repair. From this discussion, the patient could see how her training may have contributed to her pain and also disclosed that the pain started around the time she resumed dinghy racing this year.
 I should have probed a little further in regards to the patient’s training pattern. I think because she mentioned new information, relevant to the case, I felt like an overuse injury made sense and started treatment based on this clinical reasoning. However, if I had more information about her training volume, load and intensity I may have been able to provide highly individualised help and support.
I should have probed a little further in regards to the patient’s training pattern. I think because she mentioned new information, relevant to the case, I felt like an overuse injury made sense and started treatment based on this clinical reasoning. However, if I had more information about her training volume, load and intensity I may have been able to provide highly individualised help and support.
Conclusion
- Prior to this incident I have been allowing the subjective assessment to flow quite naturally and asked further questions where I felt I needed more information. However, for the time being it seems best to follow a set protocol so I don’t miss any information. I have a template subjective assessment form that I created a year ago based from a lecture.
- I will keep this template open during my note-taking so I don’t miss any significant pieces of information like I did with this patient.
Revisiting Reflection
References