22nd November – 28th November
- Hours: 15
Main Symptoms
- Fatigue
- Muscle Pain and/or Weakness
- Brain Fog
- Headaches
- Breathlessness
- Low Mood
The majority of patient symptoms align with current literature publish on long-covid. However, one study acknowledged that there are likely over 200 symptoms of long-covid (Davis, et al, 2021). Although fatigue, post-exertional malaise and cognitive dysfunction seem the most common according to this study. The NHS also have a comprehensive list of symptoms that people may experience – many of which resonate with the participants.
Initial Phone Calls
- Participants that I spoke to after the class were all quite shocked at how challenging they found the exercise class. The main reason behind this was a thought process similar to, ‘this is much less than I used to be able to do’ and ‘it shows I have a long journey ahead of me.’ Therefore, I spent a lot of time discussing how to reframe this style of thinking and celebrating the achievement of completing the exercise. For example, one participant had not tried any formal exercise since her COVID diagnosis 18 months ago. She completed the whole session and it did not exacerbate her fatigue. However, she stated that she was previously very active and would spend up to 2 hours in the gym most evenings. As a result she was deflated by how breathless she got during the session.
- I supported the participant by celebrating the successful introduction of formal exercise and there being no exacerbation of symptoms. This highlights that she is capable of doing more than what she thought. I also asked her to think of reframing her thinking style. I stated that if she is always comparing herself to pre-covid levels, any progress she makes during her recovery won’t be acknowledged or celebrated. She agreed that she needs to work on being kinder to herself and reflect on how far she has come already rather than how far she has to go, as the former is a much better motivator.
- It is expected that COVID-19 will result in a reduced tolerance to exercise (Jimeno-Almazán, et al, 2021) due to fatigue and deconditioning; however, exercise may play a role in helping to diminish these symptoms when properly delivered. Sharing this information with participant, I think, is important as it can help to set realistic expectations and encourage adherence to the programme early on. Many of them appreciate the information shared and tend to report that they know they have to take it slowly but they are just impatient.
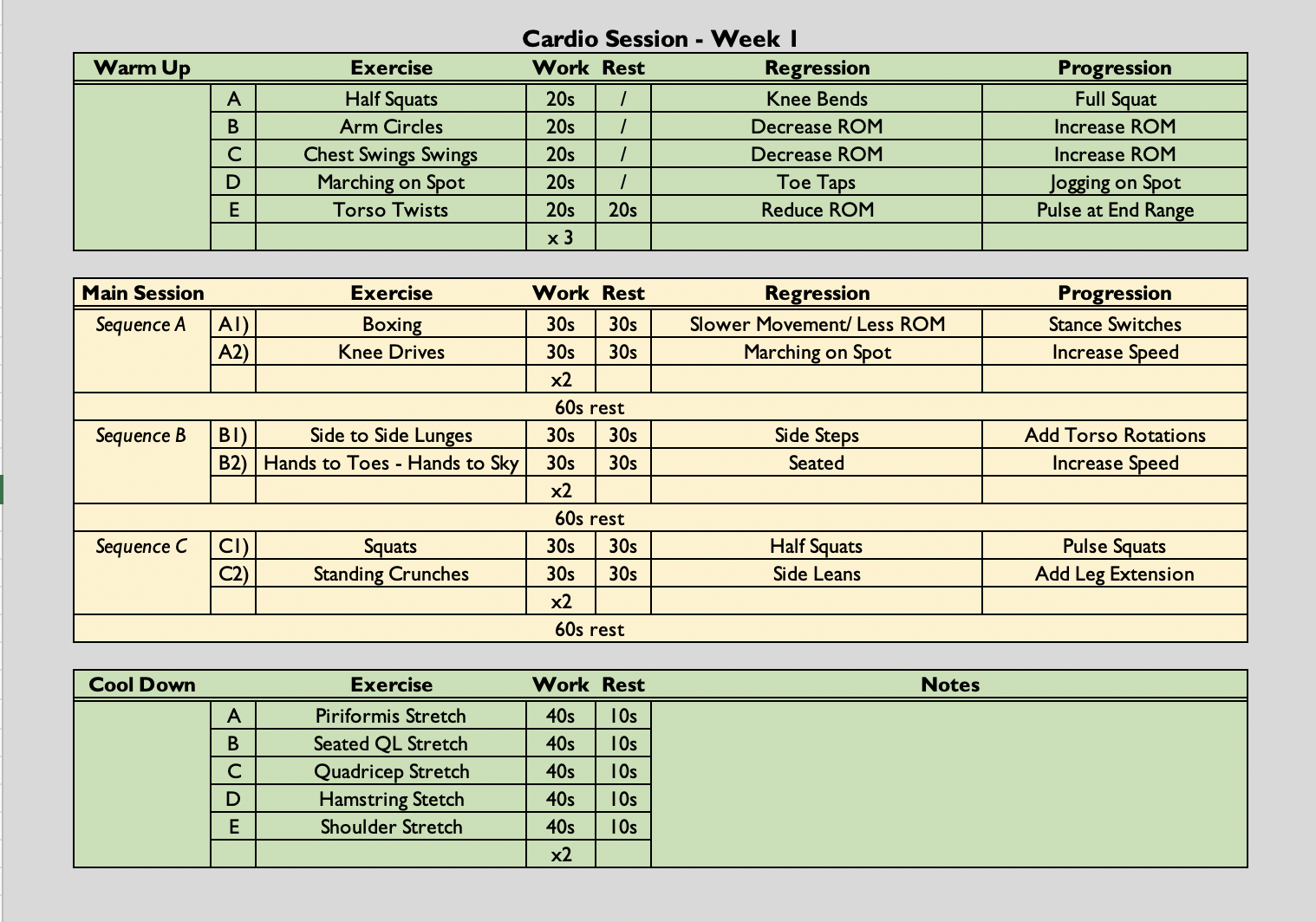
Cardio Class
- (30 seconds on to 30 seconds off (1:1) x 2, followed by a 60 second rest) x 3
- The class is always symptom-led as opposed to graded exercise therapy. Participants are free to rest when needed. They can end the class early if they have reached their limit and they can reduce the amount of sets they do if necessary.
Analysis & Evaluation
- Week 1 is quite a challenging week. I am a relative stranger to the participants so it can be difficult for them to open up or accept advice at such an early stage. However, I know that I play a crucial role in their adherence and; therefore, their chances of success on the programme. So, in a stage in early as this I work hard to get to know the individuals and build a rapport with participants as this is instrumental to adherence (Barrow and Walker, 2013). Although there are a few participants that remained quite closed during the phone calls, the majority started to open up and share personal information about how COVID has impacted them.
- One participant really didn’t respond well to exercise. The warm-up resulted in a coughing fit and the participant did very little of the exercise class (See participant update – week 5). She was very emotional on the phone and although I suggested a visit to the GP she seems to have a fractured relationship with them and did not take this advise on board.
- It seems that improving emotional wellbeing (EWB) will need to be the focus for many participants of the programme. However, one participant noted quite a substantial increase in their psychological wellbeing just from meeting other people, albeit virtually, with long covid and having a programme to help her get better. She noted that she was putting herself first for a change and it was nice not to feel alone in her recovery. Although there are both benefits and draw backs to group rehabilitation, I think this participant is likely going to respond well to the group setting. However, one of the drawbacks to group rehabilitation is, ‘what happens when the group programme doesn’t run anymore?’ Therefore, I will be mindful to really encourage independence, when using the gym and designing their own workouts as this should hopefully instil them with confidence that they can continue with their rehab independently.
- The participant that experienced a coughing fit on exertion needs to have seated alternatives to reduce intensity even further. Reassessment of suitability for the programme may need to be considered if this doesn’t help.
- It will always be easier to build a rapport with some individuals over others. However, I need to work on developing some more skills that allow me to build rapport with individuals that are a bit more closed.
Conclusion
- There is EWB training next week which I will attend to ensure I am prepared to help my participants who are struggling in this area. Being up-skilled in this area may also help me build rapport quickly.
Revisiting Reflection
- My EWB training focused on how to deal with patients who need to ‘offload’ where you typically wouldn’t know how to respond. The advice given was to always repeat back what the person has said to show you have actively listened and also to thank the participant for sharing such personal/emotional information with you. I used this technique for a participant that I was finding difficult to build a rapport with. Although not a resounding success, with the addition of some open questions, it encouraged the participant to share more. This ultimately gave me the opportunity to acknowledge what they were saying by repeating what they had said back to them.
- Sometimes I am really quick to try and give an answer or try and offer some advice – it is likely a natural instinct when you are in the position of rehabilitation – however; I need to remember I don’t have all the answers and some EWB matters are not something for me to fix but to acknowledge and onward refer if necessary.
References
- Davis, H. E., Assaf, G. S., McCorkell, L., Wei, H., Low, R. J., Re’em, Y., Redfield, S., Austin, J. P., & Akrami, A. (2021). Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine, 38, 101019. https://doi.org/10.1016/j.eclinm.2021.101019
- Jimeno-Almazán, A., Pallarés, J. G., Buendía-Romero, Á., Martínez-Cava, A., Franco-López, F., Sánchez-Alcaraz Martínez, B. J., Bernal-Morel, E., & Courel-Ibáñez, J. (2021). Post-COVID-19 Syndrome and the Potential Benefits of Exercise. International journal of environmental research and public health, 18(10), 5329. https://doi.org/10.3390/ijerph18105329
- Monna Arvinen-Barrow, & Natalie Walker. (2013). The Psychology of Sport Injury and Rehabilitation. Routledge.Monna Arvinen-Barrow, & Natalie Walker. (2013). The Psychology of Sport Injury and Rehabilitation. (pp.40-53). Routledge.